(dofetilide)
CLINICAL PHARMACOLOGY
CLINICAL PHARMACOLOGY
Mechanism of Action
Dofetilide shows Vaughan Williams Class III antiarrhythmic activity. The mechanism of action is blockade of the cardiac ion channel carrying the rapid component of the delayed rectifier potassium current, IKr. At concentrations covering several orders of magnitude, dofetilide blocks only IKr with no relevant block of the other repolarizing potassium currents (e.g., IKs, IK1). At clinically relevant concentrations, dofetilide has no effect on sodium channels (associated with Class I effect), adrenergic alpha-receptors, or adrenergic beta-receptors.
Electrophysiology
Dofetilide increases the monophasic action potential duration in a predictable, concentration-dependent manner, primarily due to delayed repolarization. This effect, and the related increase in effective refractory period, is observed in the atria and ventricles in both resting and paced electrophysiology studies. The increase in QT interval observed on the surface ECG is a result of prolongation of both effective and functional refractory periods in the His-Purkinje system and the ventricles.
Dofetilide did not influence cardiac conduction velocity and sinus node function in a variety of studies in patients with or without structural heart disease. This is consistent with a lack of effect of dofetilide on the PR interval and QRS width in patients with pre-existing heart block and/or sick sinus syndrome.
In patients, dofetilide terminates induced re-entrant tachyarrhythmias (e.g., atrial fibrillation/flutter and ventricular tachycardia) and prevents their re-induction. Dofetilide does not increase the electrical energy required to convert electrically induced ventricular fibrillation, and it significantly reduces the defibrillation threshold in patients with ventricular tachycardia and ventricular fibrillation undergoing implantation of a cardioverter-defibrillator device.
Hemodynamic Effects
In hemodynamic studies, dofetilide had no effect on cardiac output, cardiac index, stroke volume index, or systemic vascular resistance in patients with ventricular tachycardia, mild to moderate congestive heart failure or angina, and either normal or low left ventricular ejection fraction. There was no evidence of a negative inotropic effect related to dofetilide therapy in patients with atrial fibrillation. There was no increase in heart failure in patients with significant left ventricular dysfunction (see CLINICAL STUDIES, Safety in Patients with Structural Heart Disease, DIAMOND Studies). In the overall clinical program, dofetilide did not affect blood pressure. Heart rate was decreased by 4–6 bpm in studies in patients.
Pharmacokinetics, General
Absorption and Distribution: The oral bioavailability of dofetilide is >90%, with maximal plasma concentrations occurring at about 2–3 hours in the fasted state. Oral bioavailability is unaffected by food or antacid. The terminal half-life of dofetilide is approximately 10 hours; steady state plasma concentrations are attained within 2–3 days, with an accumulation index of 1.5 to 2.0. Plasma concentrations are dose proportional. Plasma protein binding of dofetilide is 60–70%, is independent of plasma concentration, and is unaffected by renal impairment. Volume of distribution is 3 L/kg.
Metabolism and Excretion:
Approximately 80% of a single dose of dofetilide is excreted in urine, of which approximately 80% is excreted as unchanged dofetilide with the remaining 20% consisting of inactive or minimally active metabolites. Renal elimination involves both glomerular filtration and active tubular secretion (via the cation transport system, a process that can be inhibited by cimetidine, trimethoprim, prochlorperazine, megestrol, ketoconazole and dolutegravir). In vitro studies with human liver microsomes show that dofetilide can be metabolized by CYP3A4, but it has a low affinity for this isoenzyme. Metabolites are formed by N-dealkylation and N-oxidation. There are no quantifiable metabolites circulating in plasma, but 5 metabolites have been identified in urine.
Pharmacokinetics in Special Populations
Renal Impairment:
In volunteers with varying degrees of renal impairment and patients with arrhythmias, the clearance of dofetilide decreases with decreasing creatinine clearance. As a result, and as seen in clinical studies, the half-life of dofetilide is longer in patients with lower creatinine clearances. Because increase in QT interval and the risk of ventricular arrhythmias are directly related to plasma concentrations of dofetilide, dosage adjustment based on calculated creatinine clearance is critically important (see DOSAGE AND ADMINISTRATION). Patients with severe renal impairment (creatinine clearance <20 mL/min) were not included in clinical or pharmacokinetic studies (see CONTRAINDICATIONS).
Hepatic Impairment:
There was no clinically significant alteration in the pharmacokinetics of dofetilide in volunteers with mild to moderate hepatic impairment (Child-Pugh Class A and B) compared to age- and weight-matched healthy volunteers. Patients with severe hepatic impairment were not studied.
Patients with Heart Disease:
Population pharmacokinetic analyses indicate that the plasma concentration of dofetilide in patients with supraventricular and ventricular arrhythmias, ischemic heart disease, or congestive heart failure are similar to those of healthy volunteers, after adjusting for renal function.
Women:
A population pharmacokinetic analysis showed that women have approximately 12–18% lower dofetilide oral clearances than men (14–22% greater plasma dofetilide levels), after correction for weight and creatinine clearance. In females, as in males, renal function was the single most important factor influencing dofetilide clearance. In normal female volunteers, hormone replacement therapy (a combination of conjugated estrogens and medroxyprogesterone) did not increase dofetilide exposure.
Dose-Response and Concentration Response for Increase in QT Interval
Increase in QT interval is directly related to dofetilide dose and plasma concentration. Figure 1 shows that the relationship in normal volunteers between dofetilide plasma concentrations and change in QTc is linear, with a positive slope of approximately 15–25 msec/(ng/mL) after the first dose and approximately 10–15 msec/(ng/mL) at Day 23 (reflecting a steady state of dosing). A linear relationship between mean QTc increase and dofetilide dose was also seen in patients with renal impairment, in patients with ischemic heart disease, and in patients with supraventricular and ventricular arrhythmias.
Figure 1: Mean QTc-Concentration Relationship in Young Volunteers Over 24 Days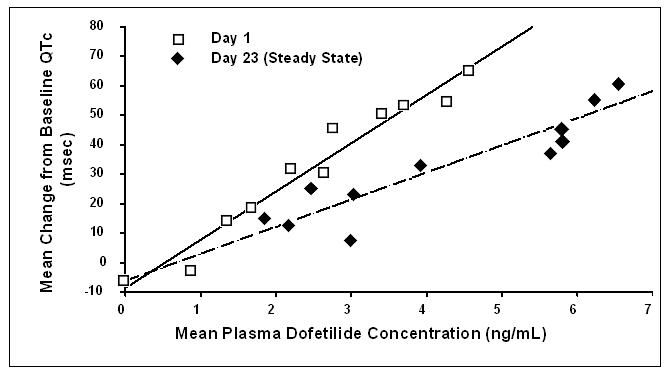
Note: The range of dofetilide plasma concentrations achieved with the 500 mcg BID dose adjusted for creatinine clearance is 1–3.5 ng/mL.
The relationship between dose, efficacy, and the increase in QTc from baseline at steady state for the two randomized, placebo-controlled studies (described further below) is shown in Figure 2. The studies examined the effectiveness of TIKOSYN in conversion to sinus rhythm and maintenance of normal sinus rhythm after conversion in patients with atrial fibrillation/flutter of >1 week duration. As shown, both the probability of a patient's remaining in sinus rhythm at six months and the change in QTc from baseline at steady state of dosing increased in an approximately linear fashion with increasing dose of TIKOSYN. Note that in these studies, doses were modified by results of creatinine clearance measurement and in-hospital QTc prolongation.
Figure 2: Relationship Between TIKOSYN Dose, QTc Increase and Maintenance of NSR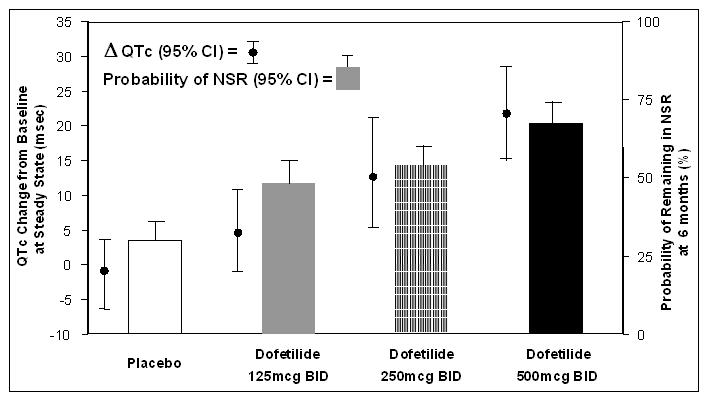
Number of patients evaluated for maintenance of NSR: 503 TIKOSYN, 174 placebo.
Number of patients evaluated for QTc change: 478 TIKOSYN, 167 placebo.
MEDICATION GUIDE
MEDICATION GUIDE
TIKOSYN® (Tee' ko sin)
(dofetilide) Capsules
Read the Medication Guide before you start taking TIKOSYN and each time you get a refill. This information does not take the place of talking with your doctor about your condition or treatment.
What is the most important information I should know about TIKOSYN?
TIKOSYN can cause serious side effects, including a type of abnormal heartbeat called Torsade de Pointes, which can lead to death.
To establish the right dose of TIKOSYN, treatment with TIKOSYN must be started in a hospital where your heart rate and kidney function will be checked for the first 3 days of treatment. It is important that when you go home, you take the exact dose of TIKOSYN that your doctor prescribed for you.
While you take TIKOSYN, always watch for signs of abnormal heartbeat.
Call your doctor and go to the hospital right away if you:
- •
- feel faint
- •
- become dizzy, or
- •
- have a fast heartbeat
What is TIKOSYN?
TIKOSYN is a prescription medicine that is used to treat an irregular heartbeat (atrial fibrillation or atrial flutter).
It is not known if TIKOSYN is safe and effective in children under 18 years of age.
Who should not take TIKOSYN?
Do not take TIKOSYN if you:
- •
- have an irregular heartbeat called long QT syndrome
- •
- have kidney problems or are on kidney dialysis
- •
- take any of these medicines:
- •
- cimetidine (TAGAMET, TAGAMET HB)1
- •
- verapamil (CALAN, CALAN SR, COVERA-HS, ISOPTIN, ISOPTIN SR, VERELAN, VERELAN PM, TARKA)1
- •
- ketoconazole (NIZORAL, XOLEGEL, EXTINA)1
- •
- trimethoprim alone (PROLOPRIM, TRIMPEX)1 or the combination of trimethoprim and sulfamethoxazole (BACTRIM, SEPTRA SULFATRIM)1
- •
- prochlorperazine (COMPAZINE, COMPO)1
- •
- megestrol (MEGACE)1
- •
- dolutegravir (TIVICAY)1
- •
- hydrochlorothiazide alone or in combination with other medicines (such as ESIDRIX, EZIDE, HYDRODIURIL, HYDRO-PAR, MICROZIDE, or ORETIC)1
- Ask your doctor if you are not sure if any of your medicines are the kind listed above.
- •
- are allergic to dofetilide in TIKOSYN. See the end of this leaflet for a complete list of ingredients in TIKOSYN.
What should I tell my doctor before taking TIKOSYN?
Before taking TIKOSYN, tell your doctor about all of your medical conditions including if you:
- •
- have heart problems
- •
- have kidney or liver problems
- •
- are pregnant or plan to become pregnant. It is not known if TIKOSYN will harm your unborn baby.
- •
- are breast-feeding or plan to breast-feed. It is not known if TIKOSYN passes into your breast milk. You and your doctor should decide if you will take TIKOSYN or breast-feed. You should not do both.
Especially tell your doctor if you take medicines to treat:
- •
- heart problems
- •
- high blood pressure
- •
- depression or other mental problems
- •
- asthma
- •
- allergies, or hay fever
- •
- skin problems
- •
- infections
Ask your doctor if you are not sure about the medicines you take. Tell your doctor about all prescription and non-prescription medicines, vitamins, dietary supplements, and any natural or herbal remedies. TIKOSYN and other medicines may affect each other, causing serious side effects. If you take TIKOSYN with certain medicines, you will be more likely to have a different type of abnormal heartbeat. See "Who should not take TIKOSYN?"
Know the medicines you take. Keep a list of your medicines and show it to your doctor and pharmacist when you get a new medicine.
How should I take TIKOSYN?
- •
- Take TIKOSYN exactly as your doctor tells you.
- •
- Do not change your TIKOSYN dose unless your doctor tells you to.
- •
- Your doctor will do tests before you start and while you take TIKOSYN.
- •
- Do not stop taking TIKOSYN until your doctor tells you to stop. If you miss a dose, just take the next dose at your regular time. Do not take 2 doses of TIKOSYN at the same time.
- •
- TIKOSYN can be taken with or without food.
- •
- If you take too much TIKOSYN, call your doctor or go to the nearest hospital emergency room right away. Take your TIKOSYN capsules with you to show to the doctor.
What are the possible side effects of TIKOSYN?
TIKOSYN can cause serious side effects, including a type of abnormal heartbeat called Torsade de Pointes, which can lead to death. See "What is the most important information I should know about TIKOSYN?"
The most common side effects of TIKOSYN include:
- •
- headache
- •
- chest pain
- •
- dizziness
Call your doctor right away if you have signs of electrolyte imbalance:
- •
- severe diarrhea
- •
- unusual sweating
- •
- vomiting
- •
- not hungry (loss of appetite)
- •
- increased thirst (drinking more than normal)
Tell your doctor if you have any side effects that bother you or do not go away.
These are not all the possible side effects of TIKOSYN. For more information, ask your doctor or pharmacist. Call your doctor for medical advice about side effects. You may report side effects to FDA at 1-800-FDA-1088.
How should I store TIKOSYN?
- •
- Store TIKOSYN between 59° to 86°F (15° to 30°C).
- •
- Keep TIKOSYN away from moisture and humidity.
- •
- Keep TIKOSYN in a tightly closed container.
- •
- Keep TIKOSYN and all medicines out of the reach of children.
General information about TIKOSYN
Medicines are sometimes prescribed for purposes other than those listed in a Medication Guide. Do not use TIKOSYN for a condition for which it was not prescribed. Do not give TIKOSYN to other people, even if they have the same symptoms you have. It may harm them.
This Medication Guide summarizes the most important information about TIKOSYN. If you would like more information, talk with your doctor. You can ask your doctor or pharmacist for information about TIKOSYN that is written for health professionals.
For more about TIKOSYN, go to www.tikosyn.com or call 1-877-TIKOSYN (1-877-845-6796).
What are the ingredients in TIKOSYN?
Active ingredient: dofetilide
Inactive ingredients:
- Capsule fill: microcrystalline cellulose, corn starch, colloidal silicon dioxide, and magnesium stearate
- Capsule shell: gelatin, titanium dioxide, and FD&C Yellow 6
- Imprinting ink: iron oxide black, shellac, n-butyl alcohol, isopropyl alcohol, propylene glycol, and ammonium hydroxide
- 1
- Listed trademarks are the property of their respective owners.
Additional Resources
Chat online with Pfizer Medical Information regarding your inquiry on a Pfizer medicine or vaccine.
Speak with a Pfizer Medical Information Professional regarding your Pfizer medicine or vaccine inquiry.
Available 9AM-5PM ET Monday to Friday; excluding holidays.
Submit a medical question for a Pfizer medicine or a vaccine.
The submission will be reviewed during our standard business hours.
To report an adverse event related to a Pfizer product and you are not part of a clinical trial* for this medication, click the link below to submit your information:
Pfizer Safety Reporting Site
*If you are involved in a clinical trial for either product, adverse events should be reported to your coordinating study site.
If you cannot use the above website to report an adverse event related to a Pfizer medication, please call (800) 438-1985.
You may also contact the U.S. Food and Drug Administration (FDA) directly to report adverse events or product quality concerns either online at www.fda.gov/medwatch or by calling (800) 332-1088.