(nafarelin acetate)
CLINICAL PHARMACOLOGY
CLINICAL PHARMACOLOGY
Nafarelin acetate is a potent agonistic analog of gonadotropin-releasing hormone (GnRH). At the onset of administration, nafarelin stimulates the release of the pituitary gonadotropins, LH and FSH, resulting in a temporary increase of gonadal steroidogenesis. Repeated dosing abolishes the stimulatory effect on the pituitary gland. Twice daily administration leads to decreased secretion of gonadal steroids by about 4 weeks; consequently, tissues and functions that depend on gonadal steroids for their maintenance become quiescent.
In children, nafarelin acetate was rapidly absorbed into the systemic circulation after intranasal administration. Maximum serum concentrations (measured by RIA) were achieved between 10 and 45 minutes. Following a single dose of 400 µg base, the observed peak concentration was 2.2 ng/mL, whereas following a single dose of 600 µg base, the observed peak concentration was 6.6 ng/mL. The average serum half-life of nafarelin following intranasal administration of a 400 µg dose was approximately 2.5 hours. It is not known and cannot be predicted what the pharmacokinetics of nafarelin will be in children given a dose above 600 µg.
In adult women, nafarelin acetate was rapidly absorbed into the systemic circulation after intranasal administration. Maximum serum concentrations (measured by RIA) were achieved between 10 and 40 minutes. Following a single dose of 200 µg base, the observed average peak concentration was 0.6 ng/mL (range 0.2 to 1.4 ng/mL), whereas following a single dose of 400 µg base, the observed average peak concentration was 1.8 ng/mL (range 0.5 to 5.3 ng/mL). Bioavailability from a 400 µg dose averaged 2.8% (range 1.2 to 5.6%). The average serum half-life of nafarelin following intranasal administration was approximately 3 hours. About 80% of nafarelin acetate was bound to plasma proteins at 4°C. Twice daily intranasal administration of 200 or 400 µg of SYNAREL in 18 healthy women for 22 days did not lead to significant accumulation of the drug. Based on the mean Cmin levels on Days 15 and 22, there appeared to be dose proportionality across the two dose levels.
After subcutaneous administration of 14C-nafarelin acetate to men, 44–55% of the dose was recovered in urine and 18.5–44.2% was recovered in feces. Approximately 3% of the administered dose appeared as unchanged nafarelin in urine. The 14C serum half-life of the metabolites was about 85.5 hours. Six metabolites of nafarelin have been identified of which the major metabolite is Tyr-D(2)-Nal-Leu-Arg-Pro-Gly-NH2(5–10). The activity of the metabolites, the metabolism of nafarelin by nasal mucosa, and the pharmacokinetics of the drug in hepatically- and renally-impaired patients have not been determined.
There appeared to be no significant effect of rhinitis, i.e., nasal congestion, on the systemic bioavailability of SYNAREL; however, if the use of a nasal decongestant for rhinitis is necessary during treatment with SYNAREL, the decongestant should not be used until at least 2 hours following dosing with SYNAREL.
When used regularly in girls and boys with central precocious puberty (CPP) at the recommended dose, SYNAREL suppresses LH and sex steroid hormone levels to prepubertal levels, affects a corresponding arrest of secondary sexual development, and slows linear growth and skeletal maturation. In some cases, initial estrogen withdrawal bleeding may occur, generally within 6 weeks after initiation of therapy. Thereafter, menstruation should cease.
In clinical studies the peak response of LH to GnRH stimulation was reduced from a pubertal response to a prepubertal response (<15 mlU/mL) within one month of treatment.
Linear growth velocity, which is commonly pubertal in children with CPP, is reduced in most children within the first year of treatment to values of 5 to 6 cm/year or less. Children with CPP are frequently taller than their chronological age peers; height for chronological age approaches normal in most children during the second or third year of treatment with SYNAREL. Skeletal maturation rate (bone age velocity—change in bone age divided by change in chronological age) is usually abnormal (greater than 1) in children with CPP; in most children, bone age velocity approaches normal (1) during the first year of treatment. This results in a narrowing of the gap between bone age and chronological age, usually by the second or third year of treatment. The mean predicted adult height increases.
In clinical trials, breast development was arrested or regressed in 82% of girls, and genital development was arrested or regressed in 100% of boys. Because pubic hair growth is largely controlled by adrenal androgens, which are unaffected by nafarelin, pubic hair development was arrested or regressed only in 54% of girls and boys.
Reversal of the suppressive effects of SYNAREL has been demonstrated to occur in all children with CPP for whom one-year post-treatment follow-up is available (n=69). This demonstration consisted of the appearance or return of menses, the return of pubertal gonadotropin and gonadal sex steroid levels, and/or the advancement of secondary sexual development. Semen analysis was normal in the two ejaculated specimens obtained thus far from boys who have been taken off therapy to resume puberty. Fertility has not been documented by pregnancies and the effect of long-term use of the drug on fertility is not known.
CLINICAL PHARMACOLOGY
Nafarelin acetate is a potent agonistic analog of gonadotropin-releasing hormone (GnRH). At the onset of administration, nafarelin stimulates the release of the pituitary gonadotropins, LH and FSH, resulting in a temporary increase of ovarian steroidogenesis. Repeated dosing abolishes the stimulatory effect on the pituitary gland. Twice daily administration leads to decreased secretion of gonadal steroids by about 4 weeks; consequently, tissues and functions that depend on gonadal steroids for their maintenance become quiescent.
Nafarelin acetate is rapidly absorbed into the systemic circulation after intranasal administration. Maximum serum concentrations (measured by RIA) were achieved between 10 and 40 minutes. Following a single dose of 200 µg base, the observed average peak concentration was 0.6 ng/mL (range 0.2 to 1.4 ng/mL), whereas following a single dose of 400 µg base, the observed average peak concentration was 1.8 ng/mL (range 0.5 to 5.3 ng/mL). Bioavailability from a 400 µg dose averaged 2.8% (range 1.2 to 5.6%). The average serum half-life of nafarelin following intranasal administration is approximately 3 hours. About 80% of nafarelin acetate is bound to plasma proteins at 4°C. Twice daily intranasal administration of 200 or 400 µg of SYNAREL in 18 healthy women for 22 days did not lead to significant accumulation of the drug. Based on the mean Cmin levels on Days 15 and 22, there appeared to be dose proportionality across the two dose levels.
After subcutaneous administration of 14C-nafarelin acetate to men, 44–55% of the dose was recovered in urine and 18.5–44.2% was recovered in feces. Approximately 3% of the administered dose appeared as unchanged nafarelin in urine. The 14C serum half-life of the metabolites was about 85.5 hours. Six metabolites of nafarelin have been identified of which the major metabolite is Tyr-D(2)-Nal-Leu-Arg-Pro-Gly-NH2(5–10). The activity of the metabolites, the metabolism of nafarelin by nasal mucosa, and the pharmacokinetics of the drug in hepatically- and renally-impaired patients have not been determined.
There appeared to be no significant effect of rhinitis, i.e., nasal congestion, on the systemic bioavailability of SYNAREL; however, if the use of a nasal decongestant for rhinitis is necessary during treatment with SYNAREL, the decongestant should not be used until at least 2 hours following dosing of SYNAREL.
In controlled clinical studies, SYNAREL at doses of 400 and 800 µg/day for 6 months was shown to be comparable to danazol, 800 mg/day, in relieving the clinical symptoms of endometriosis (pelvic pain, dysmenorrhea, and dyspareunia) and in reducing the size of endometrial implants as determined by laparoscopy. The clinical significance of a decrease in endometriotic lesions is not known at this time and, in addition, laparoscopic staging of endometriosis does not necessarily correlate with severity of symptoms.
In a single controlled clinical trial, intranasal SYNAREL (nafarelin acetate) at a dose of 400 µg per day was shown to be clinically comparable to intramuscular leuprolide depot, 3.75 mg monthly, for the treatment of the symptoms (dysmenorrhea, dyspareunia and pelvic pain) associated with endometriosis.
SYNAREL 400 µg daily induced amenorrhea in approximately 65%, 80%, and 90% of the patients after 60, 90, and 120 days, respectively. In the first, second, and third post-treatment months, normal menstrual cycles resumed in 4%, 82%, and 100%, respectively, of those patients who did not become pregnant.
At the end of treatment, 60% of patients who received SYNAREL, 400 µg/day, were symptom free, 32% had mild symptoms, 7% had moderate symptoms, and 1% had severe symptoms. Of the 60% of patients who had complete relief of symptoms at the end of treatment, 17% had moderate symptoms 6 months after treatment was discontinued, 33% had mild symptoms, 50% remained symptom free, and no patient had severe symptoms.
During the first two months use of SYNAREL, some women experience vaginal bleeding of variable duration and intensity. In all likelihood, this bleeding represents estrogen withdrawal bleeding and is expected to stop spontaneously. If vaginal bleeding continues, the possibility of lack of compliance with the dosing regimen should be considered. If the patient is complying carefully with the regimen, an increase in dose to 400 µg twice a day should be considered.
There is no evidence that pregnancy rates are enhanced or adversely affected by the use of SYNAREL.
MEDICATION GUIDE
SYNAREL
nafarelin acetate
Nasal Spray
Patient Instructions for Use
Introduction
Your doctor has prescribed SYNAREL Nasal Solution to treat your symptoms of endometriosis. This pamphlet has two purposes:
- 1.)
- to review information your doctor has given you about SYNAREL; and
- 2.)
- to give you information about how to use SYNAREL properly.
Please read this pamphlet carefully. If you still have questions after reading it or if you have questions at any time during your treatment with SYNAREL, be sure to check with your doctor.
SYNAREL is used to relieve the symptoms of endometriosis. The lining of the uterus is called the endometrium, and part of it is shed during menses. In endometriosis, endometrial tissue is also found outside the uterus and, like normal endometrial tissue, can bleed during a menstrual cycle. It is, in part, this monthly activity that causes you to have symptoms during your cycle. Most often, this out-of-place endometrial tissue is found around the uterus, ovaries, the intestine or other organs in the pelvis. Although some women with endometriosis have no symptoms, many have problems such as severe menstrual cramps, pain during sexual intercourse, low back pain, and painful bowel movements.
Endometrial tissue is affected by the body's hormones, especially estrogen, which is made by the ovaries. When estrogen levels are low, endometrial tissue shrinks (perhaps even disappears), and symptoms of endometriosis ease. SYNAREL temporarily reduces estrogen in the body and temporarily relieves the symptoms of endometriosis.
Important Information about SYNAREL
- 1.
- You should not use SYNAREL if
- •
- you are pregnant.
- •
- you are breast feeding.
- •
- you have abnormal vaginal bleeding that has not been checked into by your doctor.
- •
- you are allergic to any of the ingredients of SYNAREL (nafarelin acetate, benzalkonium chloride, acetic acid, sodium hydroxide, hydrochloric acid, sorbitol, purified water).
- 2.
- SYNAREL is a prescription medicine that should be used according to your doctor's directions. SYNAREL comes as a special nasal spray that gives a measured amount of medicine. To be effective, SYNAREL must be used every day, twice a day, for the whole treatment period.
- 3.
- It is important to use a non-hormonal method of contraception (such as diaphragm with contraceptive jelly, IUD, condoms) while taking SYNAREL. You should not use birth control pills while taking SYNAREL.
- 4.
- If you miss 1 or more doses of SYNAREL, vaginal bleeding (often called breakthrough bleeding) may occur. If you miss successive doses of SYNAREL and have not been using contraception as described above, release of an egg from the ovary (ovulation) may occur, with the possibility of pregnancy. Under these circumstances you must see your physician to make sure you are not pregnant. If you should become pregnant while using SYNAREL, you must discuss the possible risks to the fetus and the choices available to you with your physician.
- 5.
- Because SYNAREL works by temporarily reducing the body's production of estrogen, a female hormone produced by the ovary, you may have some of the same changes that normally occur at the time of menopause, when the body's production of estrogen naturally decreases. For the first two months after you start using SYNAREL, you may experience some irregular vaginal spotting or bleeding. The duration and intensity of this bleeding may vary; it may be similar to your usual menstruation, or it may be lighter or heavier. The duration may also vary from brief to prolonged. In any case, you can expect this bleeding to stop by itself. After the first two months of treatment with SYNAREL, you can expect a decrease in menstrual flow, and your periods may stop altogether. However, if you miss one or more doses of SYNAREL, you may continue to experience vaginal bleeding. If you continue to experience normal menstrual cycles after two months use of SYNAREL, you should see your doctor about the continued periods. Other changes due to decreased estrogen include hot flashes, vaginal dryness, headaches, mood changes, and decreased interest in sex. Most of these changes are caused by low estrogen levels and may occur during treatment with SYNAREL. Some patients may also experience acne, muscle pain, reduced breast size, and irritation of the tissues inside the nose. These symptoms should disappear after you stop taking the drug.
- 6.
- When you take SYNAREL, your estrogen levels will be low. Low estrogen levels can result in a small loss of mineral from bone, some of which may not be reversible. During one six-month treatment period, this small loss of mineral from bone should not be important.
There are certain conditions that may increase the possibility of the thinning of your bones when you take a drug such as SYNAREL. They are:- •
- excessive use of alcohol;
- •
- smoking;
- •
- family history of osteoporosis (thinning of the bones with fractures);
- •
- taking other medications that can cause thinning of the bones.
You should discuss the possibility of osteoporosis or thinning of the bones with your physician before starting SYNAREL. You should also be aware that repeat treatments are not recommended since they may put you at greater risk of bone thinning, particularly if you have the above conditions.
- 7.
- Depression may occur or worsen during treatment with GnRH agonists, including SYNAREL 2 mg/mL, especially in patients with a history of depression. Immediately report thoughts and behaviors of concern to your healthcare providers.
- 8.
- Severe cutaneous (skin) adverse reactions (SCARs) may happen with treatment with GnRH agonists like SYNAREL. Stop using SYNAREL and call your child’s doctor right away if your child has any of the following signs or symptoms during treatment with SYNAREL:
|
|
- 9.
- During studies, menstruation usually resumed within 2 to 3 months of stopping treatment with SYNAREL. At the end of treatment 60% of patients treated with SYNAREL were symptom free, 32% had mild symptoms, 7% had moderate symptoms and 1% had severe symptoms.
Of the 60% of patients who had complete relief of symptoms at the end of treatment, 17% had moderate symptoms at the end of the six month post-treatment period; 33% had mild symptoms; 50% were symptom free; no patient had severe symptoms.
- 10.
- Retreatment cannot be recommended since the safety of such retreatment is not known.
- 11.
- It is all right to use a nasal decongestant spray while you are being treated with SYNAREL if you follow these simple rules. Use SYNAREL first. Wait at least 2 hours after using SYNAREL before you use the decongestant spray.
- 12.
- You should avoid sneezing during or immediately after using SYNAREL, if possible, since sneezing may impair drug absorption.
Proper use of SYNAREL for Treatment of Endometriosis
- 1.
- When you start to use SYNAREL, the first dose should be taken between the second and fourth day after the beginning of your menstrual bleeding. You should continue taking SYNAREL every day as prescribed.
Do not miss a single dose. - 2.
- Unless your doctor has given you special instructions, follow the steps for using SYNAREL twice each day, about 12 hours between doses:
- •
- once in the morning in one nostril (for example, 7 a.m.)
- •
- once in the evening in the other nostril (for example, 7 p.m.)
The length of treatment is usually about 6 months, unless your doctor has given you special instructions.
- 3.
- Because it is so important that you do not miss a single dose of SYNAREL, here are some suggestions to help you remember:
- •
- Keep your SYNAREL in a place where you will be reminded to use it each morning and each evening — next to your toothbrush is one possibility.
- •
- Keep track of each dose on a calendar.
- •
- Make a note on your calendar on the day you start a new bottle of SYNAREL. You can also mark the date you started right on the bottle. Be sure to refill your prescription before the 30 days are up so you will have a new bottle on hand.
- 4.
- A bottle of SYNAREL should not be used for longer than 30 days (60 sprays). Each bottle contains sufficient quantity of nasal solution for initial priming of the pump and 30 days (60 sprays) of treatment. At the end of 30 days, a small amount of liquid will be left in the bottle. Do not try to use up that leftover amount because you might get too low a dose, which could interfere with the effectiveness of your treatment. Dispose of the bottle and do not reuse.
- 5.
- If your doctor increases your daily dose of SYNAREL, then your bottle will not last the standard 30 days. Please discuss this with your doctor to be sure that you have an adequate supply for uninterrupted treatment with SYNAREL to complete the recommended treatment period.
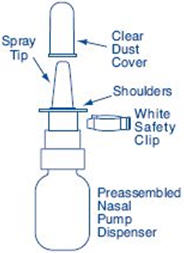
Preparation of the SYNAREL Nasal Spray unit
For use in your nose only.
Before you use SYNAREL nasal spray for the first time, you will need to prime it. This will ensure that you get the right dose of medicine each time you use it.
Important Tips about using SYNAREL
- •
- Your pump should produce a fine mist, which can only happen by a quick and firm pumping action. It is normal to see some larger droplets of liquid within the fine mist. However, if SYNAREL comes out of the pump as a thin stream of liquid instead of a fine mist, SYNAREL may not work as well, and you should talk to your pharmacist.
- •
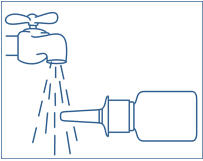
- Be sure to clean the Spray Tip before and after every use. (See Step 4). Failure to do this may result in a clogged tip that may cause you not to get the right amount of medicine that is prescribed for you.
- •
- The pump is made to deliver only a set amount of medicine, no matter how hard you pump it.
- •
- Do Not try to make the tiny hole in the spray tip larger. If the hole is made larger the pump will deliver a wrong dose of SYNAREL.
Figure A |
 |
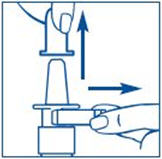
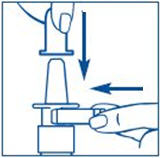
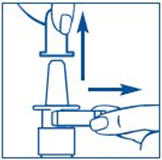
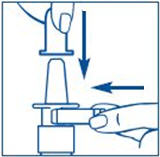
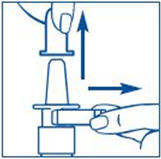
To Prime the Pump:

How to use the SYNAREL Nasal Spray unit for the treatment of Endometriosis
| |
| |
Figure G | |
 |
|
| |
| |
| |
|



It is important that you clean the spray tip before and after every use. Failure to do this may result in a clogged tip that may cause you to get the wrong dose of medicine.
Important Reminder: Treatment with SYNAREL must be uninterrupted with no missed doses to be effective. Keep out of the reach of children and use carefully as directed. |
Storage Instructions:
|
This product's label may have been updated. For current full prescribing information, please visit www.pfizer.com.
LAB-0278-10.0
Revised: November 2025
MEDICATION GUIDE | ||||
What is the most important information I should know about SYNAREL?
Call your child's doctor right away if your child has any new or worsening mental symptoms or problems while taking SYNAREL
Seizures have also happened in people who have not had any of these problems. | ||||
|
| |||
What is SYNAREL? | ||||
Do not give SYNAREL if your child:
| ||||
Before your child takes SYNAREL, tell your doctor about all of your child's medical conditions, including if they:
Tell your doctor about all the medicines your child takes, including prescription and over-the-counter medicines, vitamins, and herbal supplements. | ||||
How should your child take SYNAREL?
| ||||
What should your child avoid while taking SYNAREL?
| ||||
What are the possible side effects of SYNAREL?
| ||||
|
| |||
The side effects of SYNAREL include:
These are not all of the possible side effects of SYNAREL. Call your doctor for medical advice about side effects. You may report side effects to FDA at 1-800-FDA-1088. | ||||
General Information about the safe and effective use of SYNAREL. | ||||
What are the ingredients in SYNAREL? | ||||
Instructions for Use
SYNAREL (sin-na-rell)
(nafarelin acetate)
nasal solution
For use in the nose only.
Figure A |
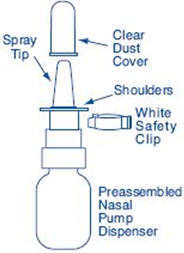 |
Before you use SYNAREL nasal spray for the first time, you will need to prime it. This will make sure that you get the right dose of medicine each time you use it. Priming only needs to be done 1 time, when you start using a new bottle of SYNAREL.
To Prime the Pump:
| |
| |
|


How to use the SYNAREL Nasal Spray for the treatment of Central Precocious Puberty
| |
| |
| |
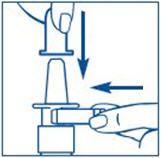
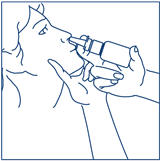
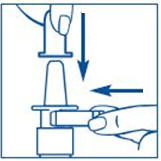
Put pressure evenly to the "shoulders" and push down quickly and firmly. Pump the sprayer 1 time, at the same time as the child sniffs in gently. Wait about 30 seconds and put one more spray in the same nostril. Repeat this process in the other nostril, for a total of four sprays. If the sprayer fails to deliver the dose, clean the spray tip (See Step 5 Clean the Spray Tip each time before and after using SYNAREL). | |
| |
|



It is important that you clean the spray tip before and after every use. Not doing this may result in a clogged tip that may cause you to get the wrong dose of medicine.
How should I store SYNAREL?
- •
- Store SYNAREL at room temperature between 59°F to 86°F (15°C to 30°C).
- •
- Store the SYNAREL bottle upright.
- •
- Keep SYNAREL out of the light.
Keep SYNAREL and all medicines out of the reach of children.
For more information call 1-800-438-1985.
This Medication Guide and Instructions for Use have been approved by the U.S. Food and Drug Administration.
Manufactured for: Pfizer Inc., 235 East 42nd Street, New York, NY, 10017
LAB-1049-4.0
Revised: November 2025
Additional Resources
Chat online with Pfizer Medical Information regarding your inquiry on a Pfizer medicine or vaccine.
Speak with a Pfizer Medical Information Professional regarding your Pfizer medicine or vaccine inquiry.
Available 9AM-5PM ET Monday to Friday; excluding holidays.
Submit a medical question for a Pfizer medicine or a vaccine.
The submission will be reviewed during our standard business hours.
To report an adverse event related to a Pfizer product and you are not part of a clinical trial* for this medication, click the link below to submit your information:
Pfizer Safety Reporting Site
*If you are involved in a clinical trial for either product, adverse events should be reported to your coordinating study site.
If you cannot use the above website to report an adverse event related to a Pfizer medication, please call (800) 438-1985.
You may also contact the U.S. Food and Drug Administration (FDA) directly to report adverse events or product quality concerns either online at www.fda.gov/medwatch or by calling (800) 332-1088.