(conjugated estrogens)
14 CLINICAL STUDIES
14 CLINICAL STUDIES
14.1 Effects on Vulvar and Vaginal Atrophy
A 12-week, prospective, randomized, double-blind placebo-controlled study was conducted to compare the safety and efficacy of 2 PREMARIN vaginal cream (PVC) regimens 0.5 g (0.3 mg CE) administered twice weekly and 0.5 g (0.3 mg CE) administered sequentially for 21 days on drug followed by 7 days off drug to matching placebo regimens in the treatment of moderate to severe symptoms of vulvar and vaginal atrophy due to menopause. The initial 12-week, double-blind, placebo-controlled phase was followed by an open-label phase to assess endometrial safety through week 52. The study randomized 423 generally healthy postmenopausal women between 44 to 77 years of age (mean 57.8 years), who at baseline had ≤ 5% superficial cells on a vaginal smear, a vaginal pH ≥ 5.0, and who identified a most bothersome moderate to severe symptom of vulvar and vaginal atrophy. The majority (92.2%) of the women were Caucasian (n = 390); 7.8% were Other (n = 33). All subjects were assessed for improvement in the mean change from baseline to Week 12 for the co-primary efficacy variables of: most bothersome symptom of vulvar and vaginal atrophy (defined as the moderate to severe symptom that had been identified by the woman as most bothersome to her at baseline); percentage of vaginal superficial cells and percentage of vaginal parabasal cells; and vaginal pH.
In the 12-week, double-blind phase, a statistically significant mean change between baseline and Week 12 in the symptom of dyspareunia was observed for both of the PREMARIN vaginal cream regimens (0.5 g daily for 21 days, then 7 days off and 0.5 g twice weekly) compared to matching placebo, see Table 3. Also demonstrated for each PREMARIN vaginal cream regimen compared to placebo was a statistically significant increase in the percentage of superficial cells at Week 12 (28%, 21/7 regimen and 26%, twice a week compared to 3% and 1% for matching placebo), a statistically significant decrease in parabasal cells (-61%, 21/7 regimen and -58%, twice a week compared to -21% and -7% for matching placebo) and statistically significant mean reduction between baseline and Week 12 in vaginal pH (-1.62, 21/7 regimen and -1.57, twice a week compared to -0.36 and -0.26 for matching placebo).
Endometrial safety was assessed by endometrial biopsy for all randomly assigned subjects at week 52. For the 155 subjects (83 on the 21/7 regimen, 72 on the twice-weekly regimen) completing the 52-week period with complete follow-up and evaluable endometrial biopsies, there were no reports of endometrial hyperplasia or endometrial carcinoma.
Dyspareunia | PVC | Placebo | PVC | Placebo |
Baseline | n | n | n | n |
Week 12 | 50 | 18 | 52 | 21 |
Change from | 50 | 18 | 52 | 21 |
P-value | <0.001 ‡ | -- | <0.001 § | -- |
14.2 Women's Health Initiative Studies
The WHI enrolled approximately 27,000 predominantly healthy postmenopausal women in two substudies to assess the risks and benefits of daily oral CE (0.625 mg)-alone or in combination with MPA (2.5 mg) compared to placebo in the prevention of certain chronic diseases. The primary endpoint was the incidence of CHD (defined as nonfatal MI, silent MI and CHD death), with invasive breast cancer as the primary adverse outcome. A "global index" included the earliest occurrence of CHD, invasive breast cancer, stroke, PE, endometrial cancer (only in the CE plus MPA substudy), colorectal cancer, hip fracture, or death due to other causes. These substudies did not evaluate the effects of CE-alone or CE plus MPA on menopausal symptoms.
WHI Estrogen-Alone Substudy
The WHI estrogen-alone substudy was stopped early because an increased risk of stroke was observed, and it was deemed that no further information would be obtained regarding the risks and benefits of estrogen-alone in predetermined primary endpoints.
Results of the estrogen-alone substudy, which included 10,739 women (average 63 years of age, range 50 to 79; 75.3% White, 15.1% Black, 6.1% Hispanic, 3.6% Other) after an average follow-up of 7.1 years, are presented in Table 4.
| |||
Event | Relative Risk | CE | Placebo |
Absolute Risk per 10,000 Women-Years | |||
CHD events‡ | 0.95 (0.78–1.16) | 54 | 57 |
Non-fatal MI‡ | 0.91 (0.73–1.14) | 40 | 43 |
CHD death‡ | 1.01 (0.71–1.43) | 16 | 16 |
All Strokes‡ | 1.33 (1.05–1.68) | 45 | 33 |
Ischemic stroke‡ | 1.55 (1.19–2.01) | 38 | 25 |
1.47 (1.06–2.06) | 23 | 15 | |
Pulmonary embolism‡ | 1.37 (0.90–2.07) | 14 | 10 |
Invasive breast cancer‡ | 0.80 (0.62–1.04) | 28 | 34 |
Colorectal cancer¶ | 1.08 (0.75–1.55) | 17 | 16 |
Hip fracture‡ | 0.65 (0.45–0.94) | 12 | 19 |
0.64 (0.44–0.93) | 11 | 18 | |
0.58 (0.47–0.72) | 35 | 59 | |
0.71 (0.64–0.80) | 144 | 197 | |
1.08 (0.88–1.32) | 53 | 50 | |
1.04 (0.88–1.22) | 79 | 75 | |
Global IndexÞ | 1.02 (0.92–1.13) | 206 | 201 |
For those outcomes included in the WHI "global index" that reached statistical significance, the absolute excess risk per 10,000 women-years in the group treated with CE-alone was 12 more strokes while the absolute risk reduction per 10,000 women-years was 7 fewer hip fractures.9 The absolute excess risk of events included in the "global index" was a non-significant 5 events per 10,000 women-years. There was no difference between the groups in terms of all-cause mortality.
No overall difference for primary CHD events (nonfatal MI, silent MI and CHD death) and invasive breast cancer incidence in women receiving CE-alone compared with placebo was reported in final centrally adjudicated results from the estrogen-alone substudy, after an average follow up of 7.1 years. See Table 4.
Centrally adjudicated results for stroke events from the estrogen-alone substudy, after an average follow-up of 7.1 years, reported no significant difference in distribution of stroke subtype or severity, including fatal strokes, in women receiving CE-alone compared to placebo. Estrogen-alone increased the risk for ischemic stroke, and this excess risk was present in all subgroups of women examined.10
Timing of the initiation of estrogen-alone therapy relative to the start of menopause may affect the overall risk benefit profile. The WHI estrogen-alone substudy stratified by age showed in women 50 to 59 years of age, a non-significant trend toward reduced risk for CHD [hazard ratio (HR) 0.63 (95% CI 0.36–1.09)] and overall mortality [HR 0.71 (95% CI 0.46–1.11)].
WHI Estrogen Plus Progestin Substudy
The WHI estrogen plus progestin substudy was stopped early. According to the predefined stopping rule, after an average follow-up of 5.6 years of treatment, the increased risk of invasive breast cancer and cardiovascular events exceeded the specified benefits included in the "global index." The absolute excess risk of events included in the "global index" was 19 per 10,000 women-years.
For those outcomes included in the WHI "global index" that reached statistical significance after 5.6 years of follow-up, the absolute excess risks per 10,000 women-years in the group treated with CE plus MPA were 7 more CHD events, 8 more strokes, 10 more PEs, and 8 more invasive breast cancers, while the absolute risk reductions per 10,000 women-years were 6 fewer colorectal cancers and 5 fewer hip fractures.
Results of the CE plus MPA substudy, which included 16,608 women (average 63 years of age, range 50 to 79; 83.9% White, 6.8% Black, 5.4% Hispanic, 3.9% Other) are presented in Table 5. These results reflect centrally adjudicated data after an average follow-up of 5.6 years.
| |||
Event | Relative Risk | CE/MPA | Placebo |
Absolute Risk per 10,000 Women-Years | |||
CHD events | 1.23 (0.99–1.53) | 41 | 34 |
Non-fatal MI | 1.28 (1.00–1.63) | 31 | 25 |
CHD death | 1.10 (0.70–1.75) | 8 | 8 |
All Strokes | 1.31 (1.03–1.68) | 33 | 25 |
Ischemic stroke | 1.44 (1.09–1.90) | 26 | 18 |
Deep vein thrombosis§ | 1.95 (1.43–2.67) | 26 | 13 |
Pulmonary embolism | 2.13 (1.45–3.11) | 18 | 8 |
Invasive breast cancer¶ | 1.24 (1.01–1.54) | 41 | 33 |
Colorectal cancer | 0.61 (0.42–0.87) | 10 | 16 |
Endometrial cancer§ | 0.81 (0.48–1.36) | 6 | 7 |
Cervical cancer§ | 1.44 (0.47–4.42) | 2 | 1 |
Hip fracture | 0.67 (0.47–0.96) | 11 | 16 |
Vertebral fractures§ | 0.65 (0.46–0.92) | 11 | 17 |
Lower arm/wrist fractures§ | 0.71 (0.59–0.85) | 44 | 62 |
Total fractures§ | 0.76 (0.69–0.83) | 152 | 199 |
Overall Mortality# | 1.00 (0.83–1.19) | 52 | 52 |
Global IndexÞ | 1.13 (1.02–1.25) | 184 | 165 |
Timing of the initiation of estrogen plus progestin therapy relative to the start of menopause may affect the overall risk benefit profile. The WHI estrogen plus progestin substudy stratified by age showed in women 50 to 59 years of age, a non-significant trend toward reduced risk for overall mortality [HR 0.69 (95% CI, 0.44–1.07)].
14.3 Women's Health Initiative Memory Study
The WHIMS estrogen-alone ancillary study of WHI enrolled 2,947 predominantly healthy hysterectomized postmenopausal women 65 to 79 years of age and older (45% were 65 to 69 years of age; 36% were 70 to 74 years of age; 19% were 75 years of age and older) to evaluate the effects of daily CE (0.625 mg)-alone on the incidence of probable dementia (primary outcome) compared to placebo.
After an average follow-up of 5.2 years, the relative risk of probable dementia for CE-alone versus placebo was 1.49 (95% CI, 0.83–2.66). The absolute risk of probable dementia for CE-alone versus placebo was 37 versus 25 cases per 10,000 women-years. Probable dementia as defined in this study included Alzheimer's disease (AD), vascular dementia (VaD) and mixed types (having features of both AD and VaD). The most common classification of probable dementia in the treatment group and the placebo group was AD. Since the ancillary study was conducted in women 65 to 79 years of age, it is unknown whether these findings apply to younger postmenopausal women [see Warnings and Precautions (5.4), and Use in Specific Populations (8.5)].
The WHIMS estrogen plus progestin ancillary study of WHI enrolled 4,532 predominantly healthy postmenopausal women 65 years of age and older (47% were 65 to 69 years of age; 35% were 70 to 74 years; 18% were 75 years of age and older) to evaluate the effects of daily CE (0.625 mg) plus MPA (2.5 mg) on the incidence of probable dementia (primary outcome) compared to placebo.
After an average follow-up of 4 years, the relative risk of probable dementia for CE plus MPA versus placebo was 2.05 (95% CI, 1.21–3.48). The absolute risk of probable dementia for CE plus MPA versus placebo was 45 versus 22 per 10,000 women-years. Probable dementia as defined in this study included AD, VaD and mixed types (having features of both AD and VaD). The most common classification of probable dementia in the treatment group and the placebo group was AD. Since the ancillary study was conducted in women 65 to 79 years of age, it is unknown whether these findings apply to younger postmenopausal women [see Warnings and Precautions (5.4), and Use in Specific Populations (8.5)].
When data from the two populations were pooled as planned in the WHIMS protocol, the reported overall relative risk for probable dementia was 1.76 (95% CI, 1.19–2.60). Differences between groups became apparent in the first year of treatment. It is unknown whether these findings apply to younger postmenopausal women [see Warnings and Precautions (5.4), and Use in Specific Populations (8.5)].
MEDICATION GUIDE
PATIENT INFORMATION
PREMARIN® (prem-uh-rin)
(Conjugated estrogens) vaginal cream
Read this PATIENT INFORMATION before you start using PREMARIN vaginal cream and read what you get each time you refill your PREMARIN vaginal cream prescription. There may be new information. This information does not take the place of talking to your healthcare provider about your menopausal symptoms or your treatment.
What is the most important information I should know about PREMARIN vaginal cream (an estrogen mixture)?
|
What is PREMARIN vaginal cream?
PREMARIN vaginal cream is a medicine that contains a mixture of estrogen hormones.
What is PREMARIN vaginal cream used for?
PREMARIN vaginal cream is used after menopause to:
- •
- Treat menopausal changes in and around the vagina
You and your healthcare provider should talk regularly about whether you still need treatment with PREMARIN vaginal cream to control these problems. - •
- Treat painful intercourse caused by menopausal changes of the vagina
Who should not use PREMARIN vaginal cream?
Do not start using PREMARIN vaginal cream if you:
- •
- Have unusual vaginal bleeding
- •
- Currently have or have had certain cancers
Estrogens may increase the chance of getting certain types of cancers, including cancer of the breast or uterus. If you have or have had cancer, talk with your healthcare provider about whether you should use PREMARIN vaginal cream. - •
- Had a stroke or heart attack
- •
- Currently have or have had blood clots
- •
- Currently have or have had liver problems
- •
- Have been diagnosed with a bleeding disorder
- •
- Are allergic to PREMARIN vaginal cream or any of its ingredients
See the end of this leaflet for a list of ingredients in PREMARIN vaginal cream.
Tell your healthcare provider:
- •
- If you have unusual vaginal bleeding
Vaginal bleeding after menopause may be a warning sign of cancer of the uterus (womb). Your healthcare provider should check any unusual vaginal bleeding to find out the cause. - •
- About all of your medical problems
Your healthcare provider may need to check you more carefully if you have certain conditions, such as asthma (wheezing), epilepsy (seizures), diabetes, migraine, endometriosis, lupus, problems with your heart, liver, thyroid, kidneys, or have high calcium levels in your blood. - •
- About all the medicines you take
This includes prescription and nonprescription medicines, vitamins, and herbal supplements. Some medicines may affect how PREMARIN vaginal cream works. PREMARIN vaginal cream may also affect how your other medicines work. - •
- If you are going to have surgery or will be on bedrest
You may need to stop using PREMARIN vaginal cream.
- •
- If you are pregnant or think you may be pregnant
PREMARIN vaginal cream is not for pregnant women
- •
- If you are breast feeding
The hormones in PREMARIN vaginal cream can pass into your breast milk.
How should I use PREMARIN vaginal cream?
PREMARIN vaginal cream is a cream that you place in your vagina with the applicator provided with the cream.
- •
- Take the dose recommended by your healthcare provider and talk to him or her about how well that dose is working for you
- •
- Estrogens should be used at the lowest dose possible for your treatment only as long as needed. You and your healthcare provider should talk regularly (for example, every 3 to 6 months) about the dose you are using and whether you still need treatment with PREMARIN vaginal cream
- •
- Step 1. Remove cap from tube.
- •
- Step 2. Screw nozzle end of applicator onto tube (Figure A).
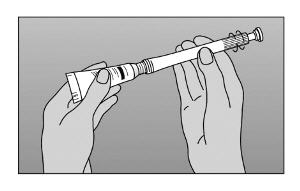 |
Figure A |
- Step 3. Gently squeeze tube from the bottom to force sufficient cream into the barrel to provide the prescribed dose. Use the marked stopping points on the applicator to measure the correct dose, as prescribed by your healthcare provider (Figure B).
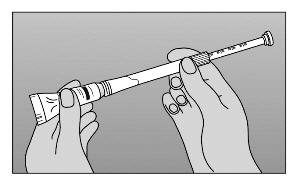 |
Figure B |
- Step 4. Unscrew applicator from tube.
- Step 5. Lie on back with knees drawn up. To deliver medication, gently insert applicator deeply into vagina and press plunger downward to its original position (Figure C).
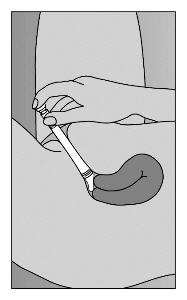 |
Figure C |
- Step 6. TO CLEANSE: Pull plunger to remove it from barrel. Wash with mild soap and warm water (Figure D).
- DO NOT BOIL OR USE HOT WATER.
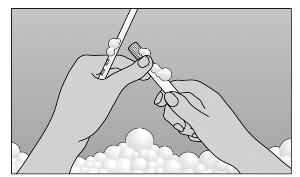 |
Figure D |
What are the possible side effects of PREMARIN vaginal cream?
PREMARIN vaginal cream is only used in and around the vagina; however, the risks associated with oral estrogens should be taken into account.
Side effects are grouped by how serious they are and how often they happen when you are treated.
Serious, but less common side effects include:
- •
- Heart attack
- •
- Stroke
- •
- Blood clots
- •
- Breast cancer
- •
- Cancer of the lining of the uterus (womb)
- •
- Cancer of the ovary
- •
- Dementia
- •
- High or low blood calcium
- •
- Gallbladder disease
- •
- Visual abnormalities
- •
- High blood pressure
- •
- High levels of fat (triglycerides) in your blood
- •
- Liver problems
- •
- Changes in your thyroid hormone levels
- •
- Fluid retention
- •
- Cancer changes of endometriosis
- •
- Enlargement of benign tumors of the uterus ("fibroids")
- •
- Severe allergic reactions
- •
- Changes in certain laboratory test results, such as high blood sugar
Call your healthcare provider right away if you get any of the following warning signs or any other unusual symptoms that concern you:
- •
- New breast lumps
- •
- Unusual vaginal bleeding
- •
- Changes in vision or speech
- •
- Sudden new severe headaches
- •
- Severe pains in your chest or legs with or without shortness of breath, weakness and fatigue
- •
- Swelling of the face, lips, and tongue with or without red itchy bumps
Common side effects of PREMARIN include:
- •
- Headache
- •
- Breast pain
- •
- Irregular vaginal bleeding or spotting
- •
- Stomach or abdominal cramps, bloating
- •
- Nausea and vomiting
- •
- Hair loss
- •
- Fluid retention
- •
- Vaginal yeast infection
- •
- Reactions from inserting PREMARIN vaginal cream, such as vaginal burning, irritation, and itching
These are not all the possible side effects of PREMARIN vaginal cream. For more information, ask your healthcare provider or pharmacist for advice about side effects. You may report side effects to FDA at 1-800-FDA-1088.
What can I do to lower my chances of getting a serious side effect with PREMARIN vaginal cream?
- •
- Talk with your healthcare provider regularly about whether you should continue using PREMARIN vaginal cream
- •
- If you have a uterus, talk to your healthcare provider about whether the addition of a progestin is right for you
The addition of a progestin is generally recommended for women with a uterus to reduce the chance of getting cancer of the uterus. See your healthcare provider right away if you get vaginal bleeding while using PREMARIN vaginal cream - •
- Have a pelvic exam, breast exam and mammogram (breast X-ray) every year unless your healthcare provider tells you something else
If members of your family have had breast cancer or if you have ever had breast lumps or an abnormal mammogram, you may need to have breast exams more often - •
- If you have high blood pressure, high cholesterol (fat in the blood), diabetes, are overweight, or if you use tobacco, you may have higher chances for getting heart disease
Ask your healthcare provider for ways to lower your chances of getting heart disease.
General information about the safe and effective use of PREMARIN vaginal cream
Medicines are sometimes prescribed for conditions that are not mentioned in patient information leaflets. Do not use PREMARIN vaginal cream for conditions for which it was not prescribed. Do not give PREMARIN vaginal cream to other people, even if they have the same symptoms you have. It may harm them.
Keep PREMARIN vaginal cream out of the reach of children.
Latex or rubber condoms, diaphragms and cervical caps may be weakened and fail when they come into contact with PREMARIN vaginal cream.
This leaflet provides a summary of the most important information about PREMARIN vaginal cream. If you would like more information, talk with your healthcare provider or pharmacist. You can ask for information about PREMARIN vaginal cream that is written for health professionals.
What are the ingredients in PREMARIN vaginal cream?
PREMARIN vaginal cream contains a mixture of conjugated estrogens, which are a mixture of sodium estrone sulfate and sodium equilin sulfate and other components, including sodium sulfate conjugates: 17 α-dihydroequilin, 17 α-estradiol, and 17 β-dihydroequilin. PREMARIN vaginal cream also contains cetyl esters wax, cetyl alcohol, white wax, glyceryl monostearate, propylene glycol monostearate, methyl stearate, benzyl alcohol, sodium lauryl sulfate, glycerin, and mineral oil.
PREMARIN vaginal cream—Each gram contains 0.625 mg conjugated estrogens, USP.
Combination package: Each contains a net wt. of 1.06 oz (30 g) tube with plastic applicator(s) calibrated in 0.5 g increments to a maximum of 2 g (NDC 0046-0872-21).
Store at 20° to 25°C (68° to 77°F); excursions permitted to 15° to 30°C (59° to 86°F) [see USP Controlled Room Temperature].
This product's labeling may have been updated. For the most recent prescribing information, please visit www.pfizer.com.
LAB-0519-8.0
Revised 04/2025
Additional Resources
Chat online with Pfizer Medical Information regarding your inquiry on a Pfizer medicine or vaccine.
Speak with a Pfizer Medical Information Professional regarding your Pfizer medicine or vaccine inquiry.
Available 9AM-5PM ET Monday to Friday; excluding holidays.
Submit a medical question for a Pfizer medicine or a vaccine.
The submission will be reviewed during our standard business hours.
To report an adverse event related to a Pfizer product and you are not part of a clinical trial* for this medication, click the link below to submit your information:
Pfizer Safety Reporting Site
*If you are involved in a clinical trial for either product, adverse events should be reported to your coordinating study site.
If you cannot use the above website to report an adverse event related to a Pfizer medication, please call (800) 438-1985.
You may also contact the U.S. Food and Drug Administration (FDA) directly to report adverse events or product quality concerns either online at www.fda.gov/medwatch or by calling (800) 332-1088.