(nicotine)
WARNINGS
WARNINGS
Nicotine from any source can be toxic and addictive. Smoking causes lung disease, cancer, and heart disease and may adversely affect pregnant women or the fetus. For any smoker, with or without concomitant disease or pregnancy, the risk of nicotine replacement in a smoking cessation program should be weighed against the hazard of continued smoking, and the likelihood of achieving cessation of smoking without nicotine replacement.
Pregnancy, Warning
Tobacco smoke, which has been shown to be harmful to the fetus, contains nicotine, hydrogen cyanide, and carbon monoxide. Nicotine has been shown in animal studies to cause fetal harm. It is therefore presumed that NICOTROL NS can cause fetal harm when administered to a pregnant woman. The effect of nicotine delivery by NICOTROL NS has not been examined in pregnancy (See PRECAUTIONS, Pregnancy). Therefore, pregnant smokers should be encouraged to attempt cessation using educational and behavioral interventions before using pharmacological approaches. If NICOTROL NS is used during pregnancy, or if the patient becomes pregnant while using it, the patient should be apprised of the potential hazard to the fetus.
Safety Note Concerning Children
The amounts of nicotine that are tolerated by adult smokers can produce signs and symptoms of poisoning and could prove fatal if NICOTROL NS is used or ingested by children or pets. Suspected nicotine poisoning in a child should be considered a medical emergency and treated immediately. A full bottle of NICOTROL NS contains 100 mg of nicotine, some of which will still be in the bottle when it is discarded. Therefore, patients should be cautioned to keep both used and unused containers of NICOTROL NS out of the reach of children and pets.
NICOTROL®NS(NICOTINE NASAL SPRAY)
Nicotrol®NS (nicotine nasal spray)
An Aid To Help You Stop Smoking
PATIENT INFORMATION
Read and follow carefully. If you have questions or want more information, ask your doctor or pharmacist.
IMPORTANT INFORMATION—Read carefully
- 1.
- NICOTROL® NS Nasal Spray is designed to help you quit smoking by reducing your urge to smoke. What causes the urge to smoke? It is the nicotine in cigarettes. NICOTROL® NS contains nicotine. Your doctor may increase or decrease dosage during the first few weeks. As your body adjusts to not smoking, your doctor will either tell you to stop using NICOTROL® NS or gradually reduce your dose.
- •
- People who use NICOTROL® NS with a comprehensive behavioral smoking cessation program are more successful in quitting smoking. This program can include support groups, counseling or specific behavior change techniques.
- 2.
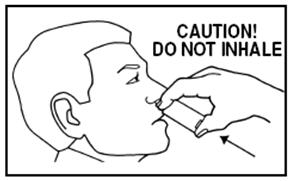
- Side Effects—During the first week or so most people experience the following side effects: hot, peppery feeling in back of throat or nose, sneezing, coughing, watery eyes, or runny nose. Wait 5 minutes before driving. Be sure to use regularly for the first week to help adjust to the side effects.
- 3.
- Because nicotine is addictive, it is possible to become dependent on the Nasal Spray. It is important to use the Nasal Spray only for as long as needed to overcome your smoking habit (as directed by your doctor). Your chance of becoming dependent on the Nasal Spray increases if you use it longer than 6 months.
WARNINGS—Read before using NICOTROL® NS


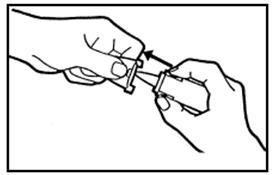
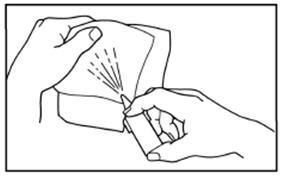
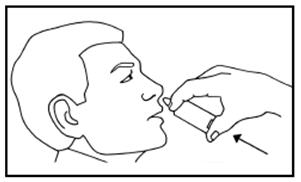
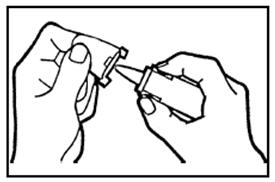
FOLLOW DIRECTIONS
BEFORE YOU USE — Read information on both sides


Additional Resources
Chat online with Pfizer Medical Information regarding your inquiry on a Pfizer medicine or vaccine.
Speak with a Pfizer Medical Information Professional regarding your Pfizer medicine or vaccine inquiry.
Available 9AM-5PM ET Monday to Friday; excluding holidays.
Submit a medical question for a Pfizer medicine or a vaccine.
The submission will be reviewed during our standard business hours.
To report an adverse event related to a Pfizer product and you are not part of a clinical trial* for this medication, click the link below to submit your information:
Pfizer Safety Reporting Site
*If you are involved in a clinical trial for either product, adverse events should be reported to your coordinating study site.
If you cannot use the above website to report an adverse event related to a Pfizer medication, please call (800) 438-1985.
You may also contact the U.S. Food and Drug Administration (FDA) directly to report adverse events or product quality concerns either online at www.fda.gov/medwatch or by calling (800) 332-1088.