(nicotine)
CLINICAL PHARMACOLOGY
CLINICAL PHARMACOLOGY
Pharmacologic Action
Nicotine, the chief alkaloid in tobacco products, binds stereo-selectively to nicotinic-cholinergic receptors at the autonomic ganglia, in the adrenal medulla, at neuromuscular junctions, and in the brain. Two types of central nervous system effects are believed to be the basis of nicotine's positively reinforcing properties. A stimulating effect is exerted mainly in the cortex via the locus ceruleus and a reward effect is exerted in the limbic system. At low doses, the stimulant effects predominate while at high doses the reward effects predominate. Intermittent intravenous administration of nicotine activates neurohormonal pathways, releasing acetylcholine, norepinephrine, dopamine, serotonin, vasopressin, beta-endorphin, growth hormone, and ACTH.
Pharmacodynamics
The cardiovascular effects of nicotine include peripheral vasoconstriction, tachycardia, and elevated blood pressure. Acute and chronic tolerance to nicotine develops from smoking tobacco or ingesting nicotine preparations. Acute tolerance (a reduction in response for a given dose) develops rapidly (less than 1 hour), but not at the same rate for different physiologic effects (skin temperature, heart rate, subjective effects). Withdrawal symptoms such as cigarette craving can be reduced in most individuals by plasma nicotine levels lower than those from smoking.
Withdrawal from nicotine in addicted individuals can be characterized by craving, nervousness, restlessness, irritability, mood lability, anxiety, drowsiness, sleep disturbances, impaired concentration, increased appetite, minor somatic complaints (headache, myalgia, constipation, fatigue), and weight gain. Nicotine toxicity is characterized by nausea, abdominal pain, vomiting, diarrhea, diaphoresis, flushing, dizziness, disturbed hearing and vision, confusion, weakness, palpitations, altered respiration and hypotension.
Both smoking and nicotine can increase circulating cortisol and catecholamines, and tolerance does not develop to the catecholamine-releasing effects of nicotine. Changes in the response to a concomitantly administered adrenergic agonist or antagonist should be watched for when nicotine intake is altered during NICOTROL NS therapy and/or smoking cessation (See PRECAUTIONS, Drug Interactions).
Pharmacokinetics
Each actuation of NICOTROL NS delivers a metered 50 microliter spray containing approximately 0.5 mg of nicotine. One dose is considered 1 mg of nicotine (2 sprays, one in each nostril).
Absorption
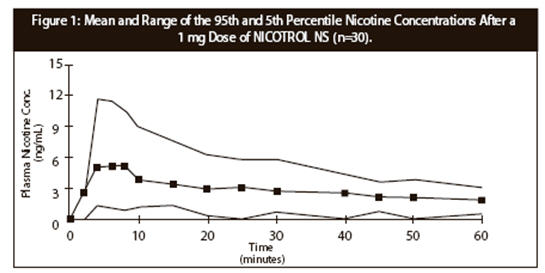
Following administration of 2 sprays of NICOTROL NS approximately 53% ± 16% (Mean ± SD) enters the systemic circulation. No significant difference in rate or extent of absorption could be seen due to the deposition of nicotine on different parts of the nasal mucosa. Plasma concentrations of nicotine obtained from 1 dose (1 mg nicotine) of NICOTROL NS rise rapidly, reaching maximum venous concentrations of 2–12 ng/mL in 4–15 minutes. The apparent absorption half-life of nicotine is approximately 3 minutes. There is wide variation among subjects in their plasma nicotine concentrations from the spray. As a result, after a 1 mg dose of spray approximately 20% of the subjects reached peak nicotine concentrations similar to those seen after smoking one cigarette (7–17 ng/mL) (See DRUG ABUSE AND DEPENDENCE). Figure 1 below plots the mean and 5th and 95th percentile nicotine concentrations after a 1 mg single dose of the nasal spray (n=30).
| Dose | Mean (ng/mL) ± SD | (Range) |
|---|---|---|
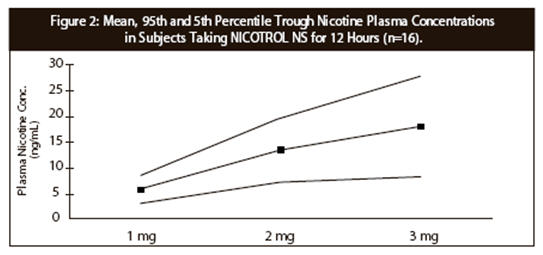
1 mg every 60 minutes (1 mg/hr) | 6 ± 3 | (1.7–12) |
1 mg every 30 minutes (2 mg/hr) | 14 ± 6 | (1.5–24) |
1 mg every 20 minutes (3 mg/hr) | 18 ± 10 | (1.2–35) |
The data from Table 1 is derived from a three-way cross-over study of repeated applications of NICOTROL NS in sixteen smokers (8 male, 8 female) ranging in age from 18 to 48 years. There is a slight deviation from dose-concentration proportionality from one dose to three doses of NICOTROL NS per hour as shown in Figure 2.
Sixteen smokers (7 males and 9 females) ranging in age from 22 to 44 years were dosed with 1 mg of NICOTROL NS every hour for 10 hours. The pharmacokinetic parameters that were obtained are presented in Table 2.
| Parameter | 1 mg (2 sprays) | (Range) |
|---|---|---|
| Cavg: average plasma nicotine concentration for the dosing interval of 10–11 hours | ||
| Cmax: maximum measured plasma concentration after last dose administration | ||
| Tmax: time of maximum plasma concentration after last dose administration | ||
Cavg (ng/mL) | 8 ± 3 | (2.5–12) |
Cmax (ng/mL) | 9 ± 3 | (3.1–14) |
Tmax (minutes) | 13 ± 5 | (10–20) |
Distribution
The volume of distribution following IV administration of nicotine is approximately 2 to 3 L/kg. Plasma protein binding of nicotine is <5%. Therefore, changes in nicotine binding from use of concomitant drugs or alterations of plasma proteins by disease states would not be expected to have significant effects on nicotine kinetics.
Metabolism
More than 20 metabolites of nicotine have been identified, all of which are less active than the parent compound. The primary urinary metabolites are cotinine (15% of the dose) and trans-3-hydroxycotinine (45% of the dose). Cotinine has a half-life of 15 to 20 hours and concentrations that exceed nicotine by 10-fold. The major site for the metabolism of nicotine is the liver. The kidney and lung are also sites of nicotine metabolism.
Elimination
About 10% of the nicotine absorbed is excreted unchanged in the urine. This may be increased to up to 30% with high urine flow rates and urinary acidification below pH 5. The average plasma clearance is about 1.2 L/min in a healthy adult smoker. The apparent elimination half-life of nicotine from NICOTROL NS is 1 to 2 hours.
Pharmacokinetic Model
The data were well described by a two-compartment model with first-order input.
Based on individual fits (N=18) the following parameters were derived after the administration of a 1 mg dose: Absorption rate constant (Ka) = 14.4 ± 7.3 hr-1 (Mean ± SD), Elimination rate constant (Ke) = 0.60 ± 0.53 hr-1, Distribution rate constants (K12) = 4.84 ± 2.57 hr-1, (K21) = 4.35 ± 2.30 hr-1, Volume of distribution over fraction absorbed (V/F) = 2.73 ± 0.82 L/kg in 8 female and 10 male adults weighing 76 ± 15 kg.
Gender Differences
Intersubject variability (50% coefficient of variation) among the pharmacokinetic parameters (AUC, Cmax and Clearance/kg) were observed for both genders. There were no differences between females or males in the kinetics of NICOTROL NS.
Renal Impairment
Progressive severity of renal impairment is associated with decreased total clearance of nicotine. Nicotine clearance was decreased by 30% on average in subjects with moderate renal impairment and 50% on average in subjects with severe renal impairment.
Hepatic Impairment
In smokers with liver cirrhosis but only mild impairment of hepatic function (Child-Pugh score 5), the pharmacokinetics of nicotine is unaffected. However, in smokers with moderately impaired liver function (Child-Pugh score 7), total clearance has been reported to be reduced on average by 40-50%. There are no data about the pharmacokinetics of nicotine in smokers with a Child-Pugh score exceeding 7, but these subjects are expected to show similar or greater effects on clearance of nicotine as patients with moderately impaired liver function.
Drug/Drug Interactions
The extent of absorption is slightly reduced (approximately 10%) in patients with the common cold/rhinitis. In patients with rhinitis the peak plasma concentration is reduced by approximately 20% (concentrations are lower by 1.5 ng/mL on average) and the time to peak concentration prolonged by approximately 30% (delayed by 7 minutes on average). The use of a nasal vasoconstrictor such as xylometazoline in patients with rhinitis will further prolong the time to peak by approximately 40% (delayed by 15 minutes on average), but the peak plasma concentration remains on average the same as those with rhinitis.
NICOTROL®NS(NICOTINE NASAL SPRAY)
Nicotrol®NS (nicotine nasal spray)
An Aid To Help You Stop Smoking
PATIENT INFORMATION
Read and follow carefully. If you have questions or want more information, ask your doctor or pharmacist.
IMPORTANT INFORMATION—Read carefully
- 1.
- NICOTROL® NS Nasal Spray is designed to help you quit smoking by reducing your urge to smoke. What causes the urge to smoke? It is the nicotine in cigarettes. NICOTROL® NS contains nicotine. Your doctor may increase or decrease dosage during the first few weeks. As your body adjusts to not smoking, your doctor will either tell you to stop using NICOTROL® NS or gradually reduce your dose.
- •
- People who use NICOTROL® NS with a comprehensive behavioral smoking cessation program are more successful in quitting smoking. This program can include support groups, counseling or specific behavior change techniques.
- 2.
- Side Effects—During the first week or so most people experience the following side effects: hot, peppery feeling in back of throat or nose, sneezing, coughing, watery eyes, or runny nose. Wait 5 minutes before driving. Be sure to use regularly for the first week to help adjust to the side effects.
- 3.
- Because nicotine is addictive, it is possible to become dependent on the Nasal Spray. It is important to use the Nasal Spray only for as long as needed to overcome your smoking habit (as directed by your doctor). Your chance of becoming dependent on the Nasal Spray increases if you use it longer than 6 months.
WARNINGS—Read before using NICOTROL® NS


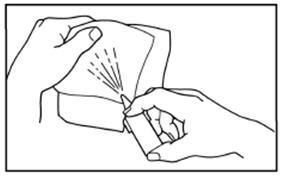
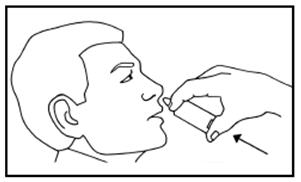
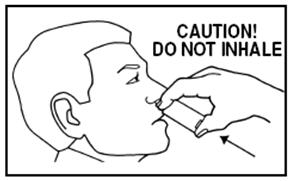
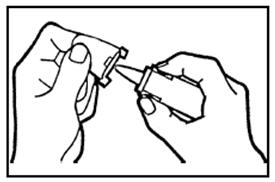
FOLLOW DIRECTIONS
BEFORE YOU USE — Read information on both sides


Additional Resources
Chat online with Pfizer Medical Information regarding your inquiry on a Pfizer medicine or vaccine.
Speak with a Pfizer Medical Information Professional regarding your Pfizer medicine or vaccine inquiry.
Available 9AM-5PM ET Monday to Friday; excluding holidays.
Submit a medical question for a Pfizer medicine or a vaccine.
The submission will be reviewed during our standard business hours.
To report an adverse event related to a Pfizer product and you are not part of a clinical trial* for this medication, click the link below to submit your information:
Pfizer Safety Reporting Site
*If you are involved in a clinical trial for either product, adverse events should be reported to your coordinating study site.
If you cannot use the above website to report an adverse event related to a Pfizer medication, please call (800) 438-1985.
You may also contact the U.S. Food and Drug Administration (FDA) directly to report adverse events or product quality concerns either online at www.fda.gov/medwatch or by calling (800) 332-1088.