(marstacimab-hncq)
HIGHLIGHTS OF PRESCRIBING INFORMATION
HIGHLIGHTS OF PRESCRIBING INFORMATIONThese highlights do not include all the information needed to use HYMPAVZI safely and effectively. See full prescribing information for HYMPAVZI. HYMPAVZI® (marstacimab-hncq) injection, for subcutaneous use Initial U.S. Approval: 2024 RECENT MAJOR CHANGESINDICATIONS AND USAGEHYMPAVZI is a tissue factor pathway inhibitor (TFPI) antagonist indicated for routine prophylaxis to prevent or reduce the frequency of bleeding episodes in adults and pediatric patients 6 years of age and older with:
DOSAGE AND ADMINISTRATION
DOSAGE FORMS AND STRENGTHSCONTRAINDICATIONSNone. (4) WARNINGS AND PRECAUTIONS
ADVERSE REACTIONSAdverse reactions reported in ≥2% of HYMPAVZI-treated patients were injection site reaction, headache, pyrexia, arthralgia, diarrhea, pruritus, and rash. (6.1) To report SUSPECTED ADVERSE REACTIONS, contact Pfizer Inc. at 1-800-438-1985 or FDA at 1-800-FDA-1088 or www.fda.gov/medwatch. See 17 for PATIENT COUNSELING INFORMATION and FDA-approved patient labeling. Revised: 6/2026 |
1 INDICATIONS AND USAGE
1 INDICATIONS AND USAGE
HYMPAVZI is indicated for routine prophylaxis to prevent or reduce the frequency of bleeding episodes in adults and pediatric patients 6 years of age and older with:
- •
- hemophilia A (congenital factor VIII deficiency) with or without factor VIII inhibitors, or
- •
- hemophilia B (congenital factor IX deficiency) with or without factor IX inhibitors.
2 DOSAGE AND ADMINISTRATION
2 DOSAGE AND ADMINISTRATION
2.1 Recommended Dosage in Adults and Pediatric Patients 12 Years of Age and Older
For subcutaneous use only.
The recommended dosage of HYMPAVZI for adults and pediatric patients 12 years of age and older is as follows:
Loading Dose
300 mg (two 150 mg subcutaneous injections)
If more than one injection is required to deliver a complete dose, administer each injection at a different injection site.
Maintenance Dose
One week after the loading dose, initiate maintenance dosing of 150 mg every week by subcutaneous injection on the same day each week, at any time of day.
Dose Adjustment During Treatment
In patients weighing greater than or equal to 50 kg, consider a dose adjustment to 300 mg subcutaneous injection weekly when control of bleeding events is judged to be inadequate by the healthcare provider. Safety and efficacy of HYMPAVZI at doses above 300 mg weekly have not been established.
If more than one injection is required to deliver a complete dose, administer each injection at a different injection site.
Missed Doses
For patients on a maintenance dose of 150 mg:
If a dose is missed, administer as soon as possible before the day of the next scheduled dose, and then resume usual 150 mg subcutaneous weekly dosing schedule (same schedule as prior to the missed dose or new schedule based on date of administration of missed dose).
If more than 13 days have passed since the last dose was administered, administer a loading dose of 300 mg by subcutaneous injection followed by a resumption of 150 mg by subcutaneous injection once weekly thereafter.
For patients on a maintenance dose of 300 mg:
If one or more doses are missed, administer a dose as soon as possible, and then resume 300 mg subcutaneous weekly dosing schedule (same schedule as prior to the missed dose or new schedule based on date of administration of missed dose).
2.2 Recommended Dosage in Pediatric Patients 6 to less than 12 Years of Age
For subcutaneous use only.
The recommended dosage of HYMPAVZI for pediatric patients 6 to less than 12 years of age is as follows:
Loading Dose
150 mg (one 150 mg subcutaneous injection or two 75 mg subcutaneous injections)
If more than one injection is required to deliver a complete dose, administer each injection at a different injection site.
Maintenance Dose
One week after the loading dose, initiate maintenance dosing of 75 mg every week by subcutaneous injection on the same day each week, at any time of day.
Dose Adjustment During Treatment
In patients weighing greater than or equal to 25 kg, consider a dose adjustment to 150 mg subcutaneous injection (one 150 mg subcutaneous injection or two 75 mg subcutaneous injections) weekly when control of bleeding events is judged to be inadequate by the healthcare provider. Safety and efficacy of HYMPAVZI at doses above 150 mg weekly have not been established in children 6 to less than 12 years of age.
If more than one injection is required to deliver a complete dose, administer each injection at a different injection site.
Missed Doses
For patients on a maintenance dose of 75 mg:
If a dose is missed, administer as soon as possible before the day of the next scheduled dose, and then resume usual 75 mg subcutaneous weekly dosing schedule (same schedule as prior to the missed dose or new schedule based on date of administration of missed dose).
If more than 13 days have passed since the last dose was administered, administer a loading dose of 150 mg by subcutaneous injection followed by a resumption of 75 mg by subcutaneous injection once weekly thereafter.
For patients on a maintenance dose of 150 mg:
If one or more doses are missed, administer a dose as soon as possible, and then resume 150 mg subcutaneous weekly dosing schedule (same schedule as prior to the missed dose or new schedule based on date of administration of missed dose).
2.3 Preparation and Administration
- •
- HYMPAVZI is intended for use under the guidance of a healthcare provider. After proper instruction in subcutaneous injection technique, a patient 12 years and older may self-inject or the patient’s caregiver may administer HYMPAVZI, if a healthcare provider determines that it is appropriate.
- •
- Refer to the Instructions for Use for complete preparation and administration instructions.
- •
- Prior to subcutaneous administration, HYMPAVZI may be removed from the refrigerator and allowed to warm at room temperature [up to 86°F (30°C)] in the carton for 15 to 30 minutes protected from direct sunlight. Do not warm by using a heat source such as hot water or a microwave. After removal of HYMPAVZI from the refrigerator, use within 7 days or discard [see How Supplied/Storage and Handling (16)].
- •
- Administer HYMPAVZI by subcutaneous injection, once weekly, at any time of the day in the abdomen or front of thigh. Other injection sites are acceptable if required. Administration of HYMPAVZI in the back of upper arm (prefilled syringe only) or buttocks (prefilled pen only) should be performed by a caregiver or healthcare professional only. HYMPAVZI should not be administered into bony areas or areas where the skin is bruised, red, tender or hard, or areas where there are scars or stretch marks. HYMPAVZI should not be injected into a vein. Rotate the injection site with each new injection.
- •
- During treatment with HYMPAVZI, other medicinal products for subcutaneous administration should, preferably, be injected at different anatomical sites.
- •
- Parenteral drug products should be inspected visually for particulate matter and discoloration prior to administration, whenever solution and container permit. HYMPAVZI is a clear and colorless to light yellow solution. Do not use if the solution is cloudy, dark yellow, or contains flakes or particles.
2.4 Changing to HYMPAVZI
Changing from prophylactic factor replacement therapy or bypassing agents to HYMPAVZI: Prior to initiation of HYMPAVZI, discontinue treatment with clotting factor concentrates (factor VIII or factor IX concentrates) or bypassing agents (e.g., recombinant FVIIa [rFVIIa] or activated prothrombin complex concentrate [aPCC]). HYMPAVZI can be initiated at any time after discontinuing clotting factor concentrates or bypassing agents.
No data are available in patients changing from other non-factor-based hemophilia medicinal products to HYMPAVZI.
2.5 Guidance on Use with Breakthrough Bleed Treatments
Factor VIII and factor IX products or bypassing agents (e.g., rFVIIa or aPCC) can be administered for the treatment of breakthrough bleeds in patients receiving HYMPAVZI. Do not use additional doses of HYMPAVZI to treat breakthrough bleeds. Healthcare providers should discuss with all patients and/or caregivers the dose and schedule of the clotting factor concentrates or bypassing agents to use, if required, while receiving HYMPAVZI prophylaxis.
When treating breakthrough bleeds with factor VIII or factor IX products or with bypassing agents, the lowest effective dose according to the product prescribing information is recommended [see Warnings and Precautions (5.1)]. Please refer to the Full Prescribing Information for the clotting factor concentrate or bypassing agent being used. For rFVIIa, a maximum dose of 90 mcg/kg body weight per dose and a maximum dosing frequency of every 2 hours is recommended. For aPCC, a maximum dose of 100 units/kg body weight within 24 hours is recommended.
2.6 Temporary Interruption for Surgery and Other Interventions
Management in the Perioperative Setting
HYMPAVZI has not been evaluated in the setting of major surgery. Patients have had minor surgical procedures without discontinuing HYMPAVZI prophylaxis in clinical studies.
For major surgery, pause HYMPAVZI at least 7 days prior and initiate management per local standard of care with clotting factor concentrate or bypassing agent and measures to manage the risk of venous thrombosis which can be elevated in the perioperative period. Consult the product information for the clotting factor concentrate or bypassing agent for dosage guidelines in patients with hemophilia undergoing major surgery. Resumption of HYMPAVZI therapy should consider the overall clinical status of the patient, including the presence of post-surgical thromboembolic risk factors, use of other hemostatic products and other concomitant medications [see Dosage and Administration (2.1)].
Management in Patients with Acute Severe Illness
There is limited experience with the use of HYMPAVZI in patients with acute severe illness. Reasons to consider temporary dose interruption of HYMPAVZI include occurrence of acute severe illness (e.g., serious infection, sepsis, trauma) in which there may be increased activation of coagulation and which the healthcare provider considers could increase the risks associated with HYMPAVZI administration. Treatment of acute severe illness should be managed per local standard of care, and continued treatment with HYMPAVZI in this situation should be weighed against the potential risks involved. Resume HYMPAVZI therapy once patient has clinically recovered [see Dosage and Administration (2.1)].
2.7 Pregnancy Testing
Verify that females of reproductive potential are not pregnant prior to initiating HYMPAVZI [see Warnings and Precautions (5.3), Use in Specific Populations (8.1, 8.3)].
2.8 Immune Tolerance Induction
The safety and efficacy of HYMPAVZI in patients receiving ongoing Immune Tolerance Induction (ITI), a desensitization strategy for the eradication of inhibitors, have not been established, and no data are available. Careful assessment of the potential benefits and risks should be performed if continuation or initiation of HYMPAVZI during ITI is considered.
3 DOSAGE FORMS AND STRENGTHS
3 DOSAGE FORMS AND STRENGTHS
HYMPAVZI (marstacimab‑hncq) is a clear and colorless to light yellow solution available as:
Prefilled Syringe
- •
- Injection: 150 mg/mL in a single-dose prefilled syringe
- •
- Injection: 75 mg/0.5 mL in a single-dose prefilled syringe
Prefilled Pen
- •
- Injection: 150 mg/mL in a single-dose prefilled pen
- •
- Injection: 75 mg/0.5 mL in a single-dose prefilled pen
4 CONTRAINDICATIONS
5 WARNINGS AND PRECAUTIONS
5 WARNINGS AND PRECAUTIONS
5.1 Thromboembolic Events
HYMPAVZI is a tissue factor pathway inhibitor (TFPI) antagonist, and may increase the risk of thromboembolic complications. Venous and arterial thromboembolic events were reported in 0.8% of patients (2/259) treated with HYMPAVZI in the open-label extension study [see Adverse Reactions (6.1)].
Patients with independent risk factors for thromboembolic events may be at increased risk of thromboembolic events with use of HYMPAVZI.
HYMPAVZI has not been studied in patients with a history of previous thromboembolic events [see Clinical Studies (14.1)]. Consider the benefit and risk of using HYMPAVZI in patients with known risk factors for thromboembolism.
Interrupt HYMPAVZI prophylaxis if diagnostic findings consistent with thromboembolism occur and manage as clinically indicated.
If factor VIII or factor IX products or bypassing agents are indicated in a patient receiving HYMPAVZI prophylaxis, the minimum effective dose according to the product label is recommended [see Dosage and Administration (2.5)].
5.2 Hypersensitivity
HYMPAVZI may cause hypersensitivity reactions (including but not limited to urticaria and pruritus). If HYMPAVZI-treated patients develop a severe hypersensitivity reaction, advise patients to discontinue HYMPAVZI and seek immediate emergency treatment.
5.3 Embryofetal Toxicity
Based on its mechanism of action, HYMPAVZI may cause fetal harm when administered to a pregnant woman [see Clinical Pharmacology (12.1)]. Advise pregnant women of the potential risk to the fetus. Advise females of reproductive potential to use effective contraception during treatment with HYMPAVZI and for 2 months after the last dose [see Use in Specific Populations (8.1, 8.3)].
5.4 Increased Laboratory Values of Fibrin D-dimer and Prothrombin Fragment 1.2
Consistent with its mechanism of action and hemostatic effect, HYMPAVZI causes an increase in fibrin D‑dimer and prothrombin fragment 1.2 [see Clinical Pharmacology (12.1, 12.2)]. Sporadic or transient increases in levels of these biomarkers above physiological values were reported with no associated safety concerns [see Clinical Pharmacology (12.2)]. Increased levels of fibrin D-dimer were seen in 10 (8.1%) pediatric patients age 6 to less than 18 years and 6 (4.4%) adults. Increased levels of prothrombin fragment 1.2 were seen in 13 (10.5%) pediatric patients age 6 to less than 18 years and 6 (4.4%) adults. For patients taking HYMPAVZI, these coagulation biomarkers may not be reliable predictive markers for clinical decision-making with suspicion of thrombosis such as deep vein thrombosis (DVT) and pulmonary embolism (PE).
6 ADVERSE REACTIONS
6 ADVERSE REACTIONS
The following clinically significant adverse reactions are described elsewhere in the labeling:
- •
- Thromboembolic Events [see Warnings and Precautions (5.1)]
- •
- Hypersensitivity [see Warnings and Precautions (5.2)]
6.1 Clinical Trials Experience
Because clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared to rates in the clinical trials of another drug and may not reflect the rates observed in practice.
The safety of HYMPAVZI was evaluated in adults and pediatric patients 6 years of age and older with severe hemophilia A (FVIII <1%) or moderately severe to severe hemophilia B (FIX ≤2%) with and without inhibitors enrolled in the BASIS and BASIS KIDS studies. A total of 259 patients received the recommended HYMPAVZI prophylaxis loading dose followed by a weekly maintenance dose starting at Day 8 administered subcutaneously [see Clinical Studies (14.1, 14.2, 14.3)]. One-hundred-thirty-five (52%) were adults (18 years of age and older), 56 (22%) were adolescents (12 to less than 18 years of age), and 68 (26%) were children (6 to less than 12 years of age). Among patients receiving HYMPAVZI, 90% were exposed for 6 months or longer and 82% were exposed for at least 1 year. The median duration of exposure across the studies was 364 days (min, max: 14, 406 days).
Table 1 summarizes the adverse reactions reported in ≥2% of patients in all age groups who received HYMPAVZI prophylaxis.
| |||
Adverse Reaction | Number of Patients 6 to less than 18 Years n (%) (N = 124) | Number of Patients 18 Years and Older n (%) (N = 135) | Number of Patients (All Age Groups) n (%) (N = 259) |
Injection site reaction† | 19 (15) | 11 (8) | 30 (12) |
Headache‡ | 9 (7) | 10 (7) | 19 (7) |
Pyrexia | 12 (10) | 3 (2) | 15 (6) |
Arthralgia | 4 (3) | 5 (4) | 9 (3) |
Diarrhea | 5 (4) | 2 (2) | 7 (3) |
Pruritus | 1 (1) | 5 (4) | 6 (2) |
Rash | 2 (2) | 3 (2) | 5 (2) |
7 DRUG INTERACTIONS
8 USE IN SPECIFIC POPULATIONS
8 USE IN SPECIFIC POPULATIONS
8.1 Pregnancy
Risk Summary
Based on its mechanism of action, HYMPAVZI may cause fetal harm when administered to a pregnant woman [see Clinical Pharmacology (12.1)]. There are no available data on HYMPAVZI use in pregnant women to evaluate for a drug-associated risk of major birth defects, miscarriage or other adverse maternal or fetal outcomes. Female animal reproduction studies have not been conducted with HYMPAVZI. Although there are no data on marstacimab‑hncq, monoclonal antibodies can be actively transported across the placenta, and marstacimab‑hncq may cause fetal harm.
The background risk of major birth defects and miscarriage for the indicated populations is unknown. All pregnancies have a background risk of birth defect, loss, or other adverse outcomes. In the U.S. general population, the estimated background risk of major birth defects and miscarriage in clinically recognized pregnancies is 2% to 4% and 15% to 20%, respectively.
8.2 Lactation
Risk Summary
There are no data on the presence of marstacimab‑hncq in either human or animal milk, the effects on the breastfed child, or the effects on milk production.
Endogenous maternal IgG and monoclonal antibodies are known to be present in human milk. The effects of local gastrointestinal exposure and limited systemic exposure in the breastfed child to marstacimab‑hncq are unknown.
The developmental and health benefits of breastfeeding should be considered along with the mother's clinical need for HYMPAVZI and any potential adverse effects on the breastfed infant from HYMPAVZI or from the underlying maternal condition.
8.3 Females and Males of Reproductive Potential
HYMPAVZI may cause fetal harm when administered to a pregnant woman [see Use in Specific Populations (8.1)].
Pregnancy Testing
Verify the pregnancy status of females of reproductive potential prior to initiating HYMPAVZI treatment.
Contraception
Females
Advise female patients of reproductive potential to use effective contraception during treatment with HYMPAVZI and for 2 months after the last dose.
8.4 Pediatric Use
The safety and effectiveness of HYMPAVZI to prevent or reduce the frequency of bleeding episodes in hemophilia A or B with and without inhibitors have been established in pediatric patients 6 years of age and older [see Clinical Studies (14.1, 14.2, 14.3)]. Use of HYMPAVZI in pediatric patients for this indication is supported by evidence from two open‑label, multi‑center studies (BASIS and BASIS KIDS). These two studies treated 56 adolescents (12 to less than 18 years of age). BASIS KIDS treated 68 children (6 to less than 12 years of age). Efficacy and adverse reaction profile were comparable between pediatric patients and adults [see Adverse Reactions (6.1) and Clinical Studies (14.1, 14.2, 14.3)]. Differences observed in steady‑state pharmacokinetic (PK) exposures between pediatric patients and adults were mostly accounted for by body weight [see Clinical Pharmacology (12.3)].
The safety and effectiveness of HYMPAVZI have not been established in pediatric patients younger than 6 years of age.
8.5 Geriatric Use
Two patients 65 years of age and older were enrolled in the clinical studies for hemophilia A or B with or without inhibitors [see Clinical Studies (14.1, 14.2)]. Clinical studies of HYMPAVZI did not include sufficient numbers of subjects 65 years of age and over to determine whether they respond differently from younger subjects.
10 OVERDOSAGE
11 DESCRIPTION
11 DESCRIPTION
Marstacimab‑hncq is a tissue factor pathway inhibitor (TFPI) antagonist, human monoclonal immunoglobulin G Type 1 (IgG1) antibody. Marstacimab‑hncq is produced by Chinese hamster ovary (CHO) cells by recombinant DNA technology and has a molecular mass of approximately 146 kDa.
HYMPAVZI (marstacimab‑hncq) injection is supplied as a sterile, preservative-free solution for subcutaneous administration. The drug product is supplied as either a single-dose prefilled syringe or as a single‑dose prefilled pen. The solution of marstacimab‑hncq is clear and colorless to light yellow with a pH of 5.8.
Each 150 mg/mL prefilled syringe or prefilled pen delivers 1 mL of HYMPAVZI. Each 1 mL of HYMPAVZI contains 150 mg of marstacimab‑hncq, and the inactive ingredients edetate disodium (0.05 mg), histidine (1.12 mg), L-histidine monohydrochloride (2.67 mg), polysorbate 80 (0.2 mg), and sucrose (85 mg), in Water for Injection, USP.
Each 75 mg/0.5 mL prefilled syringe or prefilled pen delivers 0.5 mL of HYMPAVZI. Each 0.5 mL of HYMPAVZI contains 75 mg of marstacimab‑hncq, and the inactive ingredients edetate disodium (0.03 mg), histidine (0.56 mg), L‑histidine monohydrochloride (1.34 mg), polysorbate 80 (0.1 mg), and sucrose (43 mg), in Water for Injection, USP.
12 CLINICAL PHARMACOLOGY
12 CLINICAL PHARMACOLOGY
12.1 Mechanism of Action
Marstacimab‑hncq is a human monoclonal IgG1 antibody directed against the Kunitz domain 2 (K2) of TFPI to neutralize TFPI activity and enhance coagulation. TFPI is the primary inhibitor of the extrinsic coagulation cascade and negatively regulates thrombin generation within the extrinsic pathway of coagulation by inactivating the protease functions of FXa/FVIIa/TF complex. TFPI binds to and inhibits the factor Xa active site via its second Kunitz inhibitor domain (K2).
12.2 Pharmacodynamics
For adults, adolescents and pediatric patients 6 to less than 12 years of age, marstacimab-hncq causes an increase in total TFPI (comprised of free TFPI and TFPI bound to marstacimab) and downstream biomarkers of thrombin generation such as prothrombin fragment 1+2, peak thrombin, and D‑dimer in patients with hemophilia with and without inhibitors. These changes were observed and persisted over a 7-day period following a single subcutaneous dose and were reversible after treatment discontinuation. Sporadic or transient increases in D-dimer and prothrombin fragment 1+2 above physiological values were reported in the study with no associated safety concerns.
There were no clinically relevant differences in pharmacodynamic effects between hemophilia participants with and without inhibitors or between age groups, following weekly subcutaneous administration of marstacimab‑hncq.
Drug Interaction
In Vitro Studies
In vitro studies in plasma from patients with hemophilia A and B with inhibitors demonstrated that marstacimab‑hncq in combination with rFVIIa resulted in no additive effect on thrombin generation compared to marstacimab‑hncq treatment alone. Thrombin generation increased when marstacimab‑hncq was used in combination with aPCC compared to marstacimab‑hncq treatment alone without exceeding peak thrombin levels achieved in non-hemophilic plasma treated with marstacimab‑hncq alone and in some cases were within the range reported for non-hemophilic normal plasma.
12.3 Pharmacokinetics
Estimated mean marstacimab-hncq Cmin,ss, Cmax,ss, and Cavg,ss for adults and adolescents weighing at least 25 kg following marstacimab-hncq 150 mg subcutaneous once‑weekly administration (with a loading dose of 300 mg subcutaneous), and for pediatric patients 6 to less than 12 years of age weighing at least 19 kg following marstacimab‑hncq 75 mg subcutaneous once‑weekly administration (with a loading dose of 150 mg subcutaneous) are shown in Table 2.
In adults and adolescents, the marstacimab‑hncq area under the plasma concentration-time curve (AUC) and the maximum plasma concentration (Cmax) increase in a greater than dose-proportional manner over the dose range of 100 mg to 450 mg (0.67 to 3 times the approved recommended dosage).
In adult and adolescent patients, the mean steady-state accumulation ratio for marstacimab‑hncq is approximately 4 to 5. Marstacimab‑hncq steady‑state concentrations are achieved by approximately 60 days (8th or 9th subcutaneous dose) when administered once weekly. Similar results were observed in pediatric patients 6 to less than 12 years of age.
| • Data are presented as arithmetic mean (%CV). N = number of participants | ||||||
| • Cmin,ss = minimum plasma concentration at steady state; Cmax,ss = maximum plasma concentration at steady state; Cavg,ss = average plasma concentration at steady state | ||||||
| • Adults: 18 years and older, Adolescents: 12 to less than 18 years | ||||||
Parameter | Adults | Adults | Adolescents | Adolescents | Pediatric Patients | Pediatric Patients |
N | 99 | 34 | 29 | 21 | 18 | 11 |
Cmin,ss (mcg/mL) | 13.2 (95.5%) | 16.1 (77.9%) | 30.1 (74.5%) | 35.5 (69.0%) | 10.6 (67.4%) | 16.5 (53.9%) |
Cmax,ss (mcg/mL) | 17.7 (79.6%) | 21.9 (67.7%) | 37.3 (65.9%) | 44.7 (63.5%) | 21.6 (56.4%) | 26.1 (45.4%) |
Cavg,ss (mcg/mL) | 16.1 (84.3%) | 19.8 (70.3%) | 34.8 (68.7%) | 41.4 (65.2%) | 17.1 (57.9%) | 22.4 (46.8%) |
Absorption
Bioavailability of marstacimab-hncq following subcutaneous administration is approximately 71% for adults, adolescents and pediatric patients 6 to less than 12 years of age. Median Tmax ranges from 23 to 59 hours following multiple subcutaneous administrations of marstacimab-hncq to patients with hemophilia. No clinically significant differences were seen in marstacimab-hncq bioavailability when administered subcutaneously in the arm, thigh or abdomen.
Distribution
For adults, adolescents and pediatric patients 6 to less than 12 years of age, marstacimab-hncq steady‑state apparent volume of distribution is 6.0 L in patients with hemophilia.
Elimination
Marstacimab-hncq is cleared via linear and non-linear mechanisms. Marstacimab‑hncq exhibited non‑linear pharmacokinetics due to target-mediated drug disposition (TMDD) which occurs when it forms marstacimab‑hncq/TFPI complex. Once the target becomes saturated, linear pathway (i.e., catabolism) dominates.
Based on population pharmacokinetic analysis using adult and adolescent data, 90% of marstacimab‑hncq is expected to be eliminated by the end of approximately 1 month after the last dose (median time for 50% of drug to be eliminated is approximately 7 to 11 days). Similar results were observed in pediatric patients 6 to less than 12 years of age.
Metabolism
Marstacimab‑hncq is expected to be metabolized into small peptides and amino acids by catabolic pathways in the same manner as endogenous IgG.
Specific Populations
No clinically significant differences in pharmacokinetics of marstacimab-hncq were observed in any of the age groups based on race, hemophilia type (A and B), inhibitor status and mild hepatic impairment (total bilirubin >1× to ≤1.5× ULN). In adults and adolescents, no clinically significant differences in pharmacokinetics of marstacimab‑hncq were observed based on mild renal impairment (eGFR of 60 to 89 mL/min/1.73 m2). The effects of geriatric age (>65 years), moderate to severe renal (eGFR <59 mL/min/1.73 m2) and moderate to severe hepatic (Child Pugh class B and C) impairment on marstacimab‑hncq pharmacokinetics are unknown.
Body Weight
Body weight was a significant covariate impacting the pharmacokinetics of marstacimab‑hncq. Marstacimab‑hncq exposures in adults and adolescents over the body weight range of 25 kg to 120 kg, and exposures in pediatric patients 6 to less than 12 years of age over the body weight range of 19 kg to 59 kg, show a trend for increase in exposure with decrease in body weight. However, dose adjustment based on body weight is not required for any of the age groups.
Pediatric Patients
Patients 12 to less than 18 years of age: Marstacimab‑hncq exposures (geometric mean steady‑state AUC, Cmax and Cmin) were 2.6- to 3.2‑fold higher in adolescents compared to adult patients with hemophilia; however, body weight accounts for most of these differences in exposures. These differences in PK did not translate to a clinically relevant difference in levels of the downstream pharmacodynamic marker peak thrombin between adults and adolescents.
Patients 6 to less than 12 years of age: Marstacimab‑hncq exposures (geometric mean steady‑state AUC, Cmax and Cmin) in patients with hemophilia 6 to less than 12 years of age are approximately 1.2- to 1.5‑fold higher than those in adult patients with hemophilia and approximately 1.7- to 2.8‑fold lower than those in adolescent patients with hemophilia; however, body weight accounts for most of these differences in exposure. Similar to adults and adolescents, these differences in PK do not translate to a clinically relevant difference in levels of the downstream pharmacodynamic markers between the age groups.
12.6 Immunogenicity
The observed incidence of anti-drug antibodies is highly dependent on the sensitivity and the specificity of the assay. Differences in assay methods preclude meaningful comparisons of the incidence of anti-drug antibodies (ADA) in the studies described below with the incidence of ADA in other studies, including those of marstacimab‑hncq or of other marstacimab products.
Following weekly subcutaneous marstacimab‑hncq dosing in patients with hemophilia 12 years of age and older with and without inhibitors for approximately a year in the BASIS study, 33 of the 167 (19.8%) ADA‑evaluable patients treated with marstacimab‑hncq developed ADAs. Among the 33 patients who developed ADAs, 8 patients (24.2%) developed neutralizing anti-drug antibodies (NAbs). Subjects who received marstacimab‑hncq and developed ADAs had reduced marstacimab‑hncq steady‑state concentrations, geometric mean decrease was in the range of 19% to 47%, compared to those who did not develop ADAs through the course of the treatment period.
Following weekly subcutaneous marstacimab‑hncq dosing in patients with hemophilia 6 to less than 18 years of age with and without inhibitors for approximately a year in the BASIS KIDS study, 14 of the 91 (15.4%) ADA‑evaluable patients treated with marstacimab‑hncq developed ADAs. Out of the 14 ADA‑positive patients, 4 patients were 12 to less than 18 years of age (4/24; 16.7%), 10 patients were 6 to less than 12 years of age (10/67; 14.9%). Among the 14 patients who developed ADAs, 5 patients (35.7%) developed NAbs, 1 patient was 12 to less than 18 years of age (1/3; 25.0%) and 4 patients were in 6 to less than 12 years of age (4/10; 40.0%). In subjects 12 to less than 18 years of age who received marstacimab-hncq and developed ADAs had reduced marstacimab‑hncq steady‑state concentrations, geometric mean decrease was in the range of 28% to 64%, compared to those who did not develop ADAs through the course of the treatment period. In subjects 6 to less than 12 years of age who received marstacimab-hncq and developed ADAs had increased marstacimab‑hncq steady‑state concentrations, geometric mean increase was in the range of 45% to 113%; however, exposure was comparable between ADA-positive and ADA-negative subjects after accounting for body weight.
Although lower mean marstacimab‑hncq concentrations were reported in patients aged 12 years and above who were ADA‑positive compared to those who were ADA‑negative through the course of the treatment period, there was no identified clinically significant effect of ADAs, including NAbs, on safety or efficacy of marstacimab‑hncq over the treatment duration of 12 months. Overall, the safety profile of marstacimab‑hncq was similar between patients with ADAs (including NAbs) and those without.
13 NONCLINICAL TOXICOLOGY
13 NONCLINICAL TOXICOLOGY
13.1 Carcinogenesis, Mutagenesis, Impairment of Fertility
No studies have been conducted to assess marstacimab‑hncq for the potential for carcinogenicity or mutagenicity. Marstacimab‑hncq did not affect fertility when administered as a repeat dose to male rats at doses up to 1000 mg/kg/dose and an exposure margin of 212-times the exposure at a clinical dose of 300 mg subcutaneous weekly. No effects were observed in male or female reproductive organs in the repeat‑dose toxicity studies of up to 6 months in duration in rats and 3 months in duration in cynomolgus monkeys at doses of 1000 mg/kg/dose and 500 mg/kg/dose and exposure margins at least 201- and 219-times, respectively, the AUC exposure at a clinical dose of 300 mg subcutaneous weekly.
14 CLINICAL STUDIES
14 CLINICAL STUDIES
14.1 Hemophilia A and B without Inhibitors in Adults and Pediatric Patients 12 Years of Age and Older
The efficacy of HYMPAVZI was established in 116 adults and pediatric patients (12 years of age and older and ≥35 kg) with severe hemophilia A (FVIII <1%) without FVIII inhibitors or moderately severe to severe hemophilia B (FIX ≤2%) without FIX inhibitors enrolled in the BASIS study (NCT03938792), open‑label, multi‑center, two‑phase study (observational and treatment phases). Patients with a history of coronary artery disease, venous or arterial thrombosis or ischemic disease were excluded from the study.
Following screening, patients entered a 6-month observation phase and were enrolled to two cohorts based on the factor replacement treatment they were receiving prior to study entry: on‑demand or routine prophylaxis. Patients who completed the observation phase were to receive 12 months of HYMPAVZI. Of the 116 patients who received HYMPAVZI, 33 patients were in the on‑demand treatment cohort and 83 were in the prophylactic treatment with FVIII or FIX cohort during the observation phase.
Patients received an initial 300 mg loading dose of HYMPAVZI followed by maintenance doses of 150 mg of HYMPAVZI once weekly for 12 months. Dose escalation to 300 mg of HYMPAVZI once weekly was permitted after 6 months of treatment in patients weighing ≥50 kg and experiencing 2 or more breakthrough bleeds. Fourteen (12%) underwent dose escalation.
The mean annualized bleeding rates (ABRs) for treated bleeds were 39.9 and 7.9 in the observational phase for the on-demand and prophylaxis cohorts, respectively. All patients in the on-demand cohort had one or more target joints at study entry and 36.4% had 3 or more target joints at study entry. In the routine prophylaxis cohort, 55.4% of the patients had one or more target joints at study entry and 16% had 3 or more target joints at study entry.
The efficacy of HYMPAVZI for each cohort was based upon the ABR of treated bleeds during treatment with HYMPAVZI compared to ABR during the observational phase. Other objectives of the study included evaluation of HYMPAVZI prophylaxis on the incidences of spontaneous bleeds, joint bleeds, target joint bleeds and total bleeds.
Among the 116 patients treated with HYMPAVZI in the BASIS study, the mean age was 32 years (range 13 to 66); 19 patients were 12 to less than 18 years of age and all were male. Fifty-six (56) patients were White, 58 patients were Asian, 1 patient was Black or African American and 1 patient had race information unreported; 12 patients identified as Hispanic or Latino and 104 patients identified as not Hispanic or Latino. The patient population included 91 with hemophilia A and 25 with hemophilia B.
Patients with On-Demand Factor-Based Therapy in Observational Phase
Table 3 shows the efficacy results of HYMPAVZI prophylaxis compared with on-demand factor-based therapy. HYMPAVZI prophylaxis demonstrated superiority over on-demand factor-based therapy in incidences of treated bleeds, spontaneous bleeds, joint bleeds, total bleeds and target joint bleeds.
| • p-value for the null hypothesis that the ratio = 0.5. | ||
| • The estimated mean, ratio, and confidence intervals (CIs) for the ABR come from a negative binomial regression model. | ||
| • Bleed definitions adapted based on International Society on Thrombosis and Haemostasis (ISTH) criteria: Treated bleeds = bleeds treated with FVIII or FIX; Total bleeds = bleeds treated and not treated with FVIII or FIX | ||
| • ABR = Annualized Bleeding Rate; ATP = Active Treatment Phase; CI = Confidence Interval; OD = On-Demand; OP = Observational Phase | ||
Endpoints in the Order of Testing Hierarchy | On-Demand Factor-Based Therapy During 6-Month OP (N = 33) | HYMPAVZI Prophylaxis During 12-Month ATP (N = 33) |
Treated Bleeds | ||
ABR, model-based (95% CI) | 39.9 (33.1, 48.1) | 3.2 (2.1, 4.9) |
Ratio vs. OD (95% CI) p-value | 0.08 (0.06, 0.11) <0.0001 | |
Spontaneous Bleeds, Treated | ||
ABR, model-based (95% CI) | 32.6 (25.8, 41.3) | 2.5 (1.6, 3.7) |
Ratio vs. OD (95% CI) p-value | 0.08 (0.05, 0.11) <0.0001 | |
Joint Bleeds, Treated | ||
ABR, model-based (95% CI) | 34.5 (27.8, 42.8) | 2.9 (1.8, 4.5) |
Ratio vs. OD (95% CI) p-value | 0.08 (0.06, 0.12) <0.0001 | |
Total Bleeds, Treated & Untreated | ||
ABR, model-based (95% CI) | 50.0 (42.1, 59.3) | 7.4 (5.1, 10.8) |
Ratio vs. OD (95% CI) p-value | 0.15 (0.11, 0.20) <0.0001 | |
Target Joint Bleeds, Treated | ||
ABR, model-based (95% CI) | 24.4 (18.3, 32.5) | 1.8 (1.1, 3.2) |
Ratio vs. OD (95% CI) p-value | 0.08 (0.05, 0.12) <0.0001 | |
Patients with Routine Prophylactic Factor-Based Therapy
Table 4 shows the efficacy results of HYMPAVZI prophylaxis compared with routine prophylactic factor‑based therapy. HYMPAVZI prophylaxis demonstrated non-inferiority to routine prophylactic factor‑based therapy as measured by ABR of treated bleeds as well as incidences of spontaneous bleeds, joint bleeds, target joint bleeds and total bleeds.
| • The protocol specified non-inferiority criterion (upper bound of the 95% CI for the difference) was 2.5 for treated bleeds, spontaneous bleeds, joint bleeds; 1.2 for target joint bleeds; 2.9 for total bleeds. | ||
| • The estimated mean, difference, and confidence intervals (CIs) for the ABR come from negative binomial regression model. | ||
| • Bleed definitions adapted based on ISTH criteria: Treated bleeds = bleeds treated with FVIII or FIX; Total bleeds = bleeds treated and not treated with FVIII or FIX | ||
| • ABR = Annualized Bleeding Rate; ATP = Active Treatment Phase; CI = Confidence Interval; OP = Observational Phase; RP = Routine Prophylaxis | ||
Endpoints in the Order of Testing Hierarchy | Routine Factor-Based Prophylaxis During 6-Month OP | HYMPAVZI Prophylaxis During 12-Month ATP |
Treated Bleeds | ||
ABR, model-based (95% CI) | 7.9 (5.1, 10.7) | 5.1 (3.4, 6.8) |
Difference vs. RP (95% CI) | -2.8 (-5.4, -0.2) | |
Spontaneous Bleeds, Treated | ||
ABR, model-based (95% CI) | 5.9 (3.6, 8.2) | 3.8 (2.3, 5.3) |
Difference vs. RP (95% CI) | -2.1 (-4.3, 0.0) | |
Joint Bleeds, Treated | ||
ABR, model-based (95% CI) | 5.7 (3.4, 8.0) | 4.1 (2.6, 5.7) |
Difference vs. RP (95% CI) | -1.6 (-3.7, 0.6) | |
Total Bleeds, Treated & Untreated | ||
ABR, model-based (95% CI) | 8.9 (6.0, 11.8) | 6.0 (4.1, 7.8) |
Difference vs. RP (95% CI) | -2.9 (-5.7, -0.2) | |
Target Joint Bleeds, Treated | ||
ABR, model-based (95% CI) | 3.4 (1.6, 5.2) | 2.5 (1.3, 3.8) |
Difference vs. RP (95% CI) | -0.9 (-2.4, 0.7) | |
14.2 Hemophilia A and B with Inhibitors in Adults and Pediatric Patients 12 Years of Age and Older
The efficacy of HYMPAVZI was established in 48 adults and pediatric patients (12 years of age and older and ≥35 kg) with severe hemophilia A (FVIII <1%) with FVIII inhibitors or moderately severe to severe hemophilia B (FIX ≤2%) with FIX inhibitors enrolled in the BASIS study (NCT03938792), open-label, multi-center, two-phase study (observational and treatment phases). Patients had current or history of high titer inhibitors (≥5 BU/mL) and were in need of treatment with bypassing agents in the last 6 months prior to enrollment. Patients with previous or current treatment for or history of coronary artery disease, venous or arterial thrombosis or ischemic disease were excluded from the study.
Following screening, 51 patients entered a 6‑month observation phase and received either on‑demand (N = 48) or routine prophylactic treatment (N = 3) with bypassing agents (rFVIIa or aPCC). Patients who completed the observation phase were to receive 12 months of HYMPAVZI.
Patients received an initial 300 mg loading dose of HYMPAVZI followed by maintenance doses of 150 mg of HYMPAVZI once weekly for 12 months. Dose escalation to 300 mg of HYMPAVZI once weekly was permitted after 6 months of treatment in patients weighing ≥50 kg and experiencing 2 or more breakthrough bleeds. Four (7.8%) of 51 patients underwent dose escalation.
The efficacy of HYMPAVZI was based upon the ABR of treated bleeds during treatment with HYMPAVZI compared to ABR during on-demand bypassing agent therapy during the observational phase. Other objectives of the study included evaluation of HYMPAVZI prophylaxis in comparison with on-demand bypassing agent therapy as measured by the incidences of spontaneous bleeds, joint bleeds, target joint bleeds and total bleeds.
Among the 51 male patients treated with HYMPAVZI, the mean age was 27.7 years (range 12 to 75); 25.5% of patients were 12 to less than 18 years, 74.5% were 18 years and older. In this study, 29.4% of patients were White, 54.9% were Asian, 15.7% were Black or African American, 2.0% of patients identified as Hispanic or Latino. All patients had a documented history of inhibitors (78.4% hemophilia A, 21.6% hemophilia B).
Efficacy was established in 48 patients that previously received on-demand bypassing agents before crossing over to HYMPAVZI. This population was characterized by a severe bleeding phenotype. The mean ABR for treated bleeds was 19.8 in the observational phase, prior to crossing over to weekly HYMPAVZI prophylaxis. Of the 48 patients, 70.8% had one or more target joints at study entry and 25.0% had 3 or more target joints at study entry.
Patients with On-Demand Bypassing Agent Therapy in Observational Phase
Table 5 shows the efficacy results of HYMPAVZI prophylaxis compared with on‑demand bypassing agent therapy. HYMPAVZI prophylaxis demonstrated superiority over on-demand therapy in incidences of treated bleeds, spontaneous bleeds, joint bleeds, total bleeds and target joint bleeds.
| • p-value for the null hypothesis that the ratio = 0.5. | ||
| • The estimated mean, ratio, and confidence intervals (CIs) for the ABR come from a negative binomial regression model. | ||
| • Bleed definitions adapted based on ISTH criteria: Treated bleeds = bleeds treated with bypassing agent; Total bleeds = bleeds treated and not treated with bypassing agent | ||
| • ABR = Annualized Bleeding Rate; ATP = Active Treatment Phase; CI = Confidence Interval; OD = On-Demand; OP = Observational Phase | ||
Endpoints in the Order of Testing Hierarchy | On-Demand Bypass Therapy During 6-Month OP | HYMPAVZI Prophylaxis During 12-Month ATP |
Treated Bleeds | ||
ABR, model-based (95% CI) | 19.8 (16.1, 24.3) | 1.4 (0.9, 2.3) |
Ratio vs. OD (95% CI) p-value | 0.07 (0.04, 0.12) <0.0001 | |
Spontaneous Bleeds, Treated | ||
ABR, model-based (95% CI) | 15.3 (12.1, 19.3) | 0.9 (0.5, 1.4) |
Ratio vs. OD (95% CI) p-value | 0.06 (0.04, 0.09) <0.0001 | |
Joint Bleeds, Treated | ||
ABR, model-based (95% CI) | 15.2 (11.9, 19.3) | 1.1 (0.6, 2.0) |
Ratio vs. OD (95% CI) p-value | 0.07 (0.04, 0.14) <0.0001 | |
Total Bleeds, Treated & Untreated | ||
ABR, model-based (95% CI) | 27.3 (22.5, 33.0) | 4.4 (2.7, 7.2) |
Ratio vs. OD (95% CI) p-value | 0.16 (0.10, 0.25) <0.0001 | |
Target Joint Bleeds, Treated | ||
ABR, model-based (95% CI) | 6.3 (4.3, 9.2) | 0.8 (0.4, 1.7) |
Ratio vs. OD (95% CI) p-value | 0.13 (0.06, 0.26) 0.0001 | |
14.3 Hemophilia A and B with or without Inhibitors in Pediatric Patients 6 to less than 18 Years of Age
The efficacy of HYMPAVZI was established in 57 pediatric patients 6 to less than 18 years of age with severe hemophilia A (FVIII <1%) with or without FVIII inhibitors or moderately severe to severe hemophilia B (FIX ≤2%) with or without FIX inhibitors, enrolled in the BASIS KIDS study (NCT05611801), an ongoing open‑label, multi‑center clinical study. Patients were enrolled sequentially in 2 age groups: 12 to less than 18 years of age (≥25 kg) and 6 to less than 12 years of age (≥19 kg). Patients enrolled in the study required at least 12 months of documented historical bleeding events while on on-demand or on prophylactic treatment with bypassing agents or factor replacement therapy. Patients with a history of coronary artery disease, venous or arterial thrombosis or ischemic disease were excluded from the study. The efficacy of HYMPAVZI was established in these pediatric patients who were dosed at least 12 months before the data cutoff.
Patients 6 to less than 12 years of age (N = 34) received an initial 150 mg loading dose of HYMPAVZI followed by maintenance doses of 75 mg of HYMPAVZI once weekly for 12 months. Patients 12 to less than 18 years of age (N = 23) received an initial 300 mg loading dose of HYMPAVZI followed by maintenance doses of 150 mg of HYMPAVZI once weekly for 12 months. Dose escalation to 150 mg of HYMPAVZI once weekly for patients 6 to less than 12 years of age weighing ≥25 kg or 300 mg for patients 12 to less than 18 years of age weighing ≥50 kg was allowed after 3 months for patients experiencing 2 or more breakthrough bleeds. Two (5.9%) of the 34 patients 6 to less than 12 years of age, and 3 (13%) of the 23 patients 12 to less than 18 years of age underwent dose escalation.
The efficacy of HYMPAVZI was based upon the ABR of treated bleeds during treatment with HYMPAVZI prophylaxis versus ABR of treated bleeds retrospectively collected during the 12-month historical phase. During this historical phase, in the non-inhibitor cohort (N = 36), all patients received routine prophylactic treatment with factor replacement therapy and in the inhibitor cohort (N = 21), patients received either on‑demand bypassing agents (N = 14) or routine prophylactic bypassing agents (N = 7). Other endpoints of the study included evaluation of HYMPAVZI prophylaxis as measured by the incidences of spontaneous bleeds, joint bleeds, target joint bleeds and total bleeds.
Among the 57 male patients treated with HYMPAVZI who were evaluated for efficacy, the mean age was 11 years (range 6 to 18); 59.6% of patients were 6 to less than 12 years of age and 40.4% were 12 to less than 18 years of age. In this study 35.1% of patients were White, 49.1% were Asian, 10.5% were Black or African American, 1.8% were American Indian or Alaska Native, and 3.5% race was not reported; 8.8% of patients identified as Hispanic or Latino. The patient population included 35 with hemophilia A (10 with inhibitors; 25 without inhibitors) and 22 with hemophilia B (11 with inhibitors; 11 without inhibitors).
Pediatric Patients 6 to less than 18 Years of Age with Hemophilia A or B without Inhibitors with Historic Routine Prophylactic Factor-Based Therapy
The results for the ABRs of patients without inhibitors with historic routine prophylactic factor-based therapy are shown in Table 6.
| • The estimated mean and confidence intervals (CIs) for the ABR were based on negative binomial regression model. | |||
| • The historical model-based mean ABR of treated bleeds was 3.6 (99% CI: 1.3, 5.8; median: 1.0) for pediatric patients 6 to less than 18 years old. | |||
| • ABR = Annualized Bleeding Rate; ATP = Active Treatment Phase (B7841008); CI = Confidence Interval; N = Number of patients who contributed data for analyses; Q1 = 25th percentile; Q3 = 75th percentile | |||
Endpoints | HYMPAVZI Prophylaxis During 12‑Month ATP | HYMPAVZI Prophylaxis During 12‑Month ATP | HYMPAVZI Prophylaxis During 12‑Month ATP |
Treated Bleeds | |||
Mean ABR | 1.4 | 2.6 | 1.8 |
99% CI | (0.6, 2.1) | (1.1, 4.1) | (1.1, 2.6) |
Median ABR (Q1, Q3) | 1.0 (0.0, 2.0) | 3.1 (1.0, 4.0) | 1.0 (0.5, 3.1) |
Spontaneous Bleeds, Treated | |||
Mean ABR | 0.6 | 1.1 | 0.8 |
99% CI | (0.3, 1.4) | (0.4, 3.3) | (0.4, 1.6) |
Median ABR (Q1, Q3) | 0.0 (0.0, 1.0) | 0.5 (0.0, 2.0) | 0.0 (0.0, 1.0) |
Joint Bleeds, Treated | |||
Mean ABR | 0.6 | 1.7 | 1.0 |
99% CI | (0.2, 0.9) | (0.5, 2.9) | (0.4, 1.6) |
Median ABR (Q1, Q3) | 0.0 (0.0, 1.0) | 1.5 (0.0, 3.1) | 0.5 (0.0, 1.6) |
Total Bleeds, Treated & Untreated | |||
Mean ABR | 2.3 | 2.9 | 2.5 |
99% CI | (1.5, 3.6) | (1.7, 4.9) | (1.8, 3.6) |
Median ABR (Q1, Q3) | 2.0 (1.0, 3.0) | 3.1 (1.0, 4.1) | 2.1 (1.0, 4.0) |
Target Joint Bleeds, Treated | |||
Mean ABR | 0.1 | 0.5 | 0.2 |
99% CI | (0.0, 0.6) | (0.1, 2.5) | (0.0, 0.9) |
Median ABR (Q1, Q3) | 0.0 (0.0, 0.0) | 0.0 (0.0, 0.0) | 0.0 (0.0, 0.0) |
Pediatric Patients 6 to less than 18 Years of Age with Hemophilia A or B with Inhibitors
The results for the ABRs of patients with inhibitors and prior on-demand bypassing therapy are shown in Table 7.
| • The estimated mean and confidence intervals (CIs) for the ABR were based on negative binomial regression model. | |||
| • The historical model‑based mean ABR of treated bleeds was 18.9 (99% CI: 14.2, 25.2; median: 15.5) for pediatric patients 6 to less than 18 years old. | |||
| • ABR = Annualized Bleeding Rate; ATP = Active Treatment Phase (B7841008); CI = Confidence Interval; N = Number of patients who contributed data for analyses; Q1 = 25th percentile; Q3 = 75th percentile | |||
Endpoints | HYMPAVZI Prophylaxis During 12‑Month ATP | HYMPAVZI Prophylaxis During 12‑Month ATP | HYMPAVZI Prophylaxis During 12‑Month ATP |
Treated Bleeds | |||
Mean ABR | 1.3 | 1.6 | 1.4 |
99% CI | (0.5, 3.4) | (0.2, 10.8) | (0.5, 4.5) |
Median ABR (Q1, Q3) | 1.0 (0.0, 3.0) | 0.0 (0.0, 2.0) | 0.0 (0.0, 2.0) |
Spontaneous Bleeds, Treated | |||
Mean ABR | 0.7 | 1.4 | 1.1 |
99% CI | (0.1, 5.8) | (0.1, 22.3) | (0.2, 6.4) |
Median ABR (Q1, Q3) | 0.0 (0.0, 2.1) | 0.0 (0.0, 1.0) | 0.0 (0.0, 1.0) |
Joint Bleeds, Treated | |||
Mean ABR | 0.9 | 1.6 | 1.2 |
99% CI | (0.3, 2.7) | (0.2, 10.8) | (0.3, 4.6) |
Median ABR (Q1, Q3) | 1.0 (0.0, 1.0) | 0.0 (0.0, 2.0) | 0.0 (0.0, 1.0) |
Total Bleeds, Treated & Untreated | |||
Mean ABR | 1.4 | 1.7 | 1.6 |
99% CI | (0.6, 3.3) | (0.2, 12.3) | (0.6, 4.2) |
Median ABR (Q1, Q3) | 1.0 (0.0, 3.0) | 0.0 (0.0, 2.0) | 1.0 (0.0, 2.0) |
Target Joint Bleeds, Treated | |||
Mean ABR | 0.6 | 1.2 | 0.9 |
99% CI | (0.1, 4.5) | (0, 93.3) | (0.1, 7.5) |
Median ABR (Q1, Q3) | 0.0 (0.0, 1.0) | 0.0 (0.0, 0.0) | 0.0 (0.0, 0.0) |
16 HOW SUPPLIED/STORAGE AND HANDLING
16 HOW SUPPLIED/STORAGE AND HANDLING
16.1 How Supplied
HYMPAVZI (marstacimab-hncq) injection is a sterile, preservative-free, clear and colorless to light yellow solution for subcutaneous administration available as a single-dose prefilled syringe or pen in the following presentations:
Presentation | Package Size | NDC Number |
Single-dose prefilled syringe: | ||
75 mg/0.5 mL | Carton of 1 | NDC 0069-1575-01 |
150 mg/mL | Carton of 1 | NDC 0069-1510-01 |
Single-dose prefilled pen: | ||
75 mg/0.5 mL | Carton of 1 | NDC 0069-0775-01 |
150 mg/mL | Carton of 1 | NDC 0069-2151-01 |
Prefilled Syringe
Each carton contains a single-dose prefilled syringe (Type I glass) with a plunger stopper (chlorobutyl elastomer) and a stainless steel 27 gauge, ½ inch staked needle with a rigid needle shield (thermoplastic elastomer).
Prefilled Pen
Each carton contains a single-dose prefilled pen with needle guard. The syringe inside the pen is made from Type I glass with a plunger stopper (chlorobutyl elastomer) and a stainless steel 27 gauge, ½ inch staked needle with a rigid needle shield (thermoplastic elastomer).
HYMPAVZI is not made with natural rubber latex.
16.2 Recommended Storage and Handling
- •
- Store refrigerated at 36°F to 46°F (2°C to 8°C) in the original carton to protect from light.
- •
- If needed, HYMPAVZI may be stored one time at room temperature [up to 86°F (30°C)] in its original carton to protect from light for up to 7 days. Once stored at room temperature, do not return to the refrigerator and discard after 7 days.
- •
- Do not freeze.
- •
- Do not shake.
17 PATIENT COUNSELING INFORMATION
17 PATIENT COUNSELING INFORMATION
- •
- Advise the patient and/or caregivers to read the FDA-approved patient labeling (Patient Information and Instructions for Use).
- •
- Ensure that patients and caregivers who will administer HYMPAVZI receive appropriate training and instruction on the proper storage, use and handling of HYMPAVZI from a healthcare professional.
Thromboembolic Events
Inform patients and/or caregivers that HYMPAVZI increases coagulation potential. Discuss the appropriate dosing of concomitant agents such as FVIII or FIX with the patient prior to starting on HYMPAVZI prophylaxis. Advise the patient to discontinue HYMPAVZI and seek immediate medical attention if any signs or symptoms of thromboembolism occur [see Warnings and Precautions (5.1)].
Hypersensitivity
Inform patients and/or caregivers that hypersensitivity reactions such as rash and pruritus are possible. Advise patients to discontinue HYMPAVZI and seek immediate emergency treatment if a severe hypersensitivity reaction occurs [see Warnings and Precautions (5.2)].
Pregnancy
Advise female patients of reproductive potential to use effective contraception during treatment with HYMPAVZI and for 2 months after the last dose. Advise patients to report known pregnancies [see Warnings and Precautions (5.3), Use in Specific Populations (8.1, 8.3)].
This product’s labeling may have been updated. For the most recent prescribing information, please visit www.pfizer.com.

US License No. 2001
Distributed by
Pfizer Labs
Division of Pfizer Inc.
New York, NY 10001
LAB-1556-4.0
Medication Guide
| This Patient Information has been approved by the U.S. Food and Drug Administration. Revised: 6/2026 | |||
PATIENT INFORMATION HYMPAVZI® (him-PAV-zee) (marstacimab-hncq) injection, for subcutaneous use | |||
Important information:
| |||
What is HYMPAVZI? HYMPAVZI is a prescription medicine used regularly to prevent or reduce the frequency of bleeding episodes in adults and children 6 years of age and older with:
It is not known if HYMPAVZI is safe and effective in people receiving ongoing Immune Tolerance Induction (ITI). It is not known if HYMPAVZI is safe and effective in children younger than 6 years of age. | |||
Before using HYMPAVZI, tell your healthcare provider about all of your medical conditions, including if you:
Tell your healthcare provider about all the medicines you take, including prescription medicines, over‑the‑counter medicines, vitamins, and herbal supplements. Know the medicines you take. Keep a list of them to show your healthcare provider and pharmacist when you get a new medicine. | |||
How should I use HYMPAVZI? See the detailed “Instructions for Use” that comes with your HYMPAVZI for information on how to inject a dose of HYMPAVZI, and how to properly throw away (dispose of) used HYMPAVZI prefilled syringe or HYMPAVZI prefilled pen.
| |||
What are the possible side effects of HYMPAVZI? HYMPAVZI may cause serious side effects, including:
| |||
|
| ||
| |||
|
| ||
The most common side effects of HYMPAVZI include: | |||
|
| ||
These are not all of the possible side effects of HYMPAVZI. Call your doctor for medical advice about side effects. You may report side effects to FDA at 1-800-FDA-1088. | |||
How should I store HYMPAVZI?
Keep HYMPAVZI and all medicines out of the reach of children. | |||
General information about the safe and effective use of HYMPAVZI. Medicines are sometimes prescribed for purposes other than those listed in a Patient Information leaflet. Do not use HYMPAVZI for a condition for which it was not prescribed. Do not give HYMPAVZI to other people, even if they have the same symptoms that you have. It may harm them. You can ask your pharmacist or healthcare provider for information about HYMPAVZI that is written for health professionals. | |||
What are the ingredients in HYMPAVZI? Active ingredient: marstacimab‑hncq Inactive ingredients: edetate disodium, histidine, L-histidine monohydrochloride, polysorbate 80, sucrose, and water for injection | |||
This product's labeling may have been updated. For the most recent prescribing information, please visit www.pfizer.com.
| |||

Instructions For Use
INSTRUCTIONS FOR USE
HYMPAVZI® (him-PAV-zee)
(marstacimab-hncq)
injection, for subcutaneous use
150 mg single-dose prefilled syringe
This Instructions for Use contains information on how to inject HYMPAVZI.
Read this Instructions for Use carefully before using HYMPAVZI Prefilled Syringe and each time you get a refill prescription as there may be new information.
People 12 years of age and older, or their caregiver, may inject HYMPAVZI if your healthcare provider decides it is appropriate. Your healthcare provider should show you or your caregiver how to prepare and inject HYMPAVZI before you use it for the first time. Do not inject yourself or someone else until you have been shown how to inject HYMPAVZI.
Important Information You Need to Know Before Injecting HYMPAVZI
- •
- Each HYMPAVZI Prefilled Syringe is a Single-Dose Prefilled Syringe (called “Syringe” in this Instructions for Use). The HYMPAVZI Prefilled Syringe contains 150 mg of HYMPAVZI for injection under the skin (subcutaneously).
- •
- Do not inject HYMPAVZI into a vein.
- •
- To help you remember when to inject HYMPAVZI, you can mark your calendar ahead of time. Call your healthcare provider if you or your caregiver have any questions about the right way to inject HYMPAVZI, or call the helpline at 1‑888‑496‑7289 (1‑888 HYMPAV‑Z).
- •
- Use HYMPAVZI exactly as prescribed by your healthcare provider.
- •
- HYMPAVZI is not made with natural rubber latex.
Storing HYMPAVZI
- •
- Store HYMPAVZI in a refrigerator at 36°F to 46°F (2°C to 8°C).
- •
- Store HYMPAVZI in the original carton to protect from light.
- •
- If needed, HYMPAVZI may be stored one time at room temperature, up to 86°F (30°C) in the original carton for up to 7 days. Do not return HYMPAVZI to the refrigerator after storing at room temperature.
- •
- Throw away (dispose of) HYMPAVZI that has been left out of the refrigerator for more than 7 days.
- •
- Do not freeze HYMPAVZI.
- •
- Do not shake HYMPAVZI.
- •
- Do not use past the expiration date (Exp) printed on the HYMPAVZI Prefilled Syringe.
- •
- Keep HYMPAVZI and all medicines out of the reach of children.
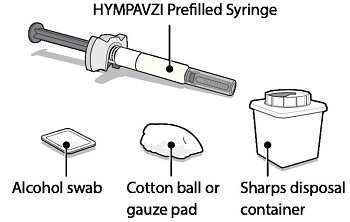
Supplies Needed For HYMPAVZI Injection
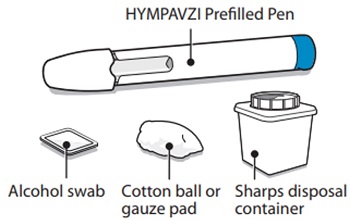
Gather the following supplies on a clean flat surface:
Included in the carton:
- •
- 1 HYMPAVZI Prefilled Syringe
Not included in the carton:
- •
- 1 alcohol swab
- •
- 1 cotton ball or gauze pad
- •
- 1 FDA-cleared sharps disposal container for Syringe disposal (see “Step 11 – Disposal of Syringe” and “Safe Syringe Disposal” information section)
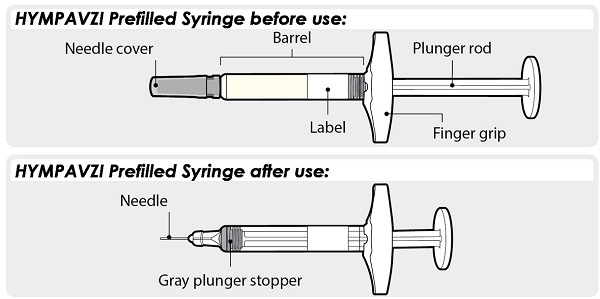
HYMPAVZI Prefilled Syringe
Always hold HYMPAVZI Prefilled Syringe by the barrel to prevent damage.
Preparing to Inject HYMPAVZI
Step 1 – Getting Ready
- •
- Remove the Syringe from its carton and keep out of direct sunlight.
- •
- Make sure the name HYMPAVZI appears on the carton and Syringe label.
- •
- Check the Syringe for any visible damage such as cracks or leaks.
- •
- Wash and dry your hands.
- •
- Do not remove the needle cover until you are ready to inject.
- •
- Throw away (dispose of) the Syringe if it is damaged, or if the Syringe or the carton containing the Syringe has been dropped.
- •
- Do not use the Syringe if:
- o
- it has been stored in direct light. Exposure to room light during dose preparation and injection is acceptable.
- o
- it has been frozen or thawed, or it has been out of the refrigerator for more than 7 days.
Note: For a more comfortable injection, allow the Syringe to warm at room temperature up to 86°F (30°C) in the carton away from direct sunlight for about 15 to 30 minutes.
Do not use any other methods to warm up the Syringe, such as warming the Syringe in a microwave or hot water.
Step 2 – Check Expiration Date
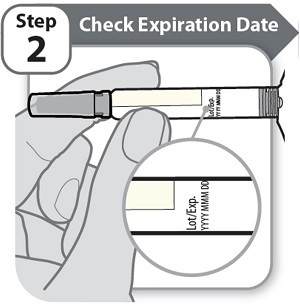
- •
- Check the expiration date (Exp) printed on the Syringe label.
- •
- Do not use if the expiration date (Exp) has passed.
Step 3 – Check Medicine
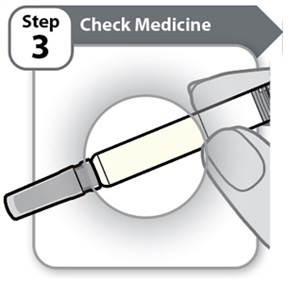
- •
- Gently tilt the Syringe back and forth.
- •
- Look carefully at the medicine in the Syringe.
- o
- The medicine should be clear and colorless to light yellow.
- o
- Do not use the Syringe if the medicine is cloudy, dark yellow, or contains flakes or particles.
Note: It is normal to see air bubbles in the Syringe.
If you have any questions about the medicine, contact your healthcare provider.
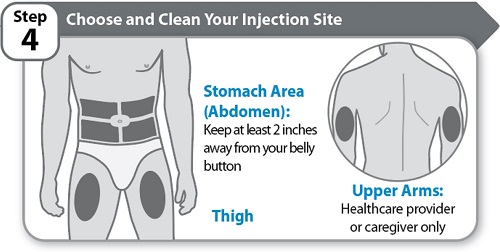
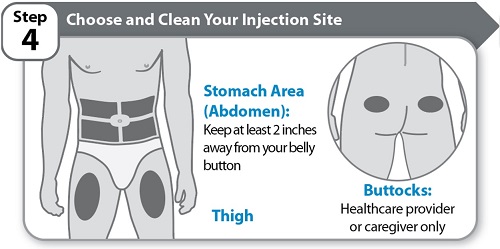
Step 4 – Choose and Clean Your Injection Site
- •
- Choose an injection site on your stomach area (abdomen) or front of thigh unless a different site has been suggested by your healthcare provider. HYMPAVZI may also be injected into the back of your upper arms by a healthcare provider or caregiver only. Keep at least 2 inches away from your belly button.
- •
- Change (rotate) the injection site each time you give yourself an injection of HYMPAVZI and away from any other medicine given under your skin. You may use the same area of your body but be sure to choose a different injection site in that area.
- •
- Clean the injection site with soap and water, or an alcohol swab.
- •
- Allow the site to air dry. Do not touch, fan, or blow on the cleaned injection site.
- •
- Do not inject HYMPAVZI into bony areas or areas on your skin that are bruised, red, sore (tender) or hard. Avoid injecting into areas with scars or stretch marks.
- •
- Do not inject HYMPAVZI into a vein.
- •
- Do not inject HYMPAVZI through your clothes.
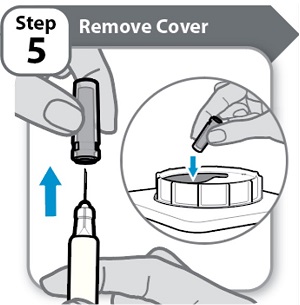
Step 5 – Remove Cover
- •
- Hold the Syringe by the barrel.
- •
- Pull the needle cover straight off carefully.
- •
- Put the needle cover into an FDA-cleared sharps disposal container right away. You will not need it again.
- •
- Do not touch the needle or let it touch any surfaces.
Note: It is normal to see a few drops of medicine at the needle tip.
Caution: Handle the Syringe with care to avoid an accidental needle injury.
Injecting HYMPAVZI
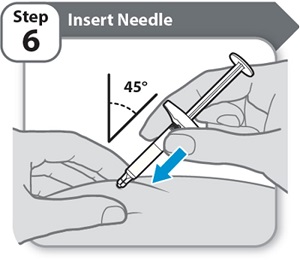
Step 6 – Insert Needle
- •
- Pinch your cleaned skin between your thumb and fingers to create a firm surface.
- •
- Fully insert the needle into your skin at a 45° angle, as shown. Do not hold or push on the plunger while inserting the needle.
Keep your skin pinched throughout the injection.
Caution: If you change your mind where to inject after inserting the needle into your skin, you will need to throw away (dispose of) the Syringe and get a new HYMPAVZI Prefilled Syringe.
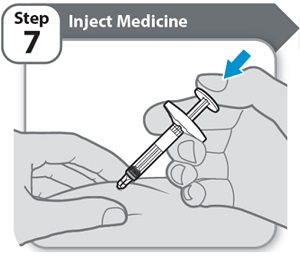
Step 7 – Inject Medicine
- •
- Slowly inject all of HYMPAVZI by gently pushing the plunger rod all the way down, until the barrel is empty.
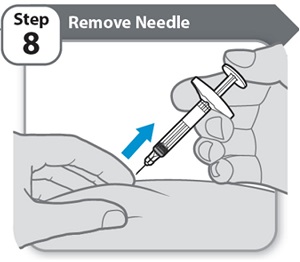
Step 8 – Remove Needle
- •
- Pull the needle and Syringe out of your skin at the same angle as inserted.
Note: If you see a small drop of medicine on your skin, wait a little longer before removing the needle when you give your next injection.
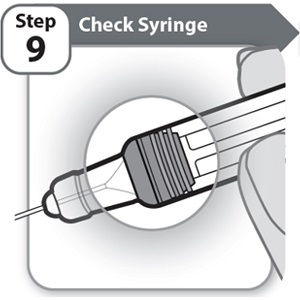
Step 9 – Check Syringe
- •
- Check the Syringe to make sure the gray plunger stopper is in the position shown.
If the gray plunger stopper is not in the position shown, this means you have not received a full dose. Call your healthcare provider for help.
Never re-insert the needle.
Do not inject another dose.
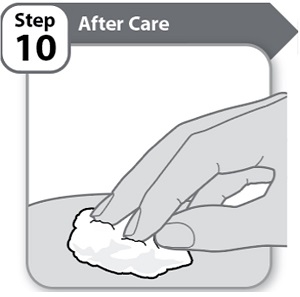
Step 10 – After Care
- •
- Press lightly on the injection site for a few seconds with a clean cotton ball or gauze pad if you see a drop of blood.
- •
- Do not rub the area.
Note: If bleeding does not stop, contact your healthcare provider.
Note: If your prescribed dose requires 2 injections of HYMPAVZI, repeat steps 1-10. Change (rotate) the injection site each time you give yourself an injection of HYMPAVZI. You may use the same area of your body but be sure to choose a different injection site in that area.
- •
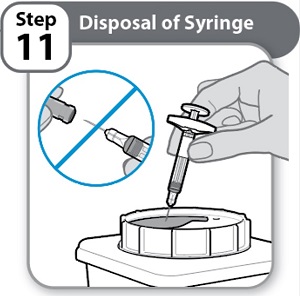
- Put the used Syringe in an FDA-cleared sharps disposal container right away after use.
Never re-cap the needle.
- •
- Do not throw away (dispose of) Syringes in the household trash.
Note: If you do not have an FDA-cleared sharps disposal container, please see the “Safe Syringe Disposal” information section.
- •
- Always throw away (dispose of) Syringes in a sharps disposal container. Do not dispose of Syringes in the household trash.
- •
- If you do not have an FDA-cleared sharps disposal container, you may use a household container that:
- o
- is made of heavy-duty plastic,
- o
- can be closed with a tight-fitting, puncture-resistant lid, without sharps being able to come out,
- o
- is upright and stable during use,
- o
- is leak-resistant, and
- o
- is properly labeled to warn of hazardous waste inside the container.
- •
- When your sharps disposal container is almost full, you will need to follow your community guidelines for the right way to throw away (dispose of) your sharps disposal container. There may be state or local laws about how you should throw away used needles and syringes. For more information about safe sharps disposal, and for specific information about safe sharps disposal for the state you live in, go to the FDA’s website at: http://www.fda.gov/safesharpsdisposal.
- •
- Do not recycle your used sharps disposal container.

US License No. 2001
Distributed by
Pfizer Labs
Division of Pfizer Inc.
New York, NY 10001
LAB-1576-3.0
For more information, go to www.pfizer.com or call 1-800-438-1985.
This Instructions for Use has been approved by the U.S. Food and Drug Administration. Revised: 6/2026
INSTRUCTIONS FOR USE
HYMPAVZI® (him-PAV-zee)
(marstacimab-hncq)
injection, for subcutaneous use
150 mg single-dose prefilled pen
This Instructions for Use contains information on how to inject HYMPAVZI.
Read this Instructions for Use carefully before using HYMPAVZI Prefilled Pen and each time you get a refill prescription as there may be new information.
People 12 years of age and older, or their caregiver, may inject HYMPAVZI if your healthcare provider decides it is appropriate. Your healthcare provider should show you or your caregiver how to prepare and inject HYMPAVZI before you use it for the first time. Do not inject yourself or someone else until you have been shown how to inject HYMPAVZI.
Important Information You Need to Know Before Injecting HYMPAVZI
- •
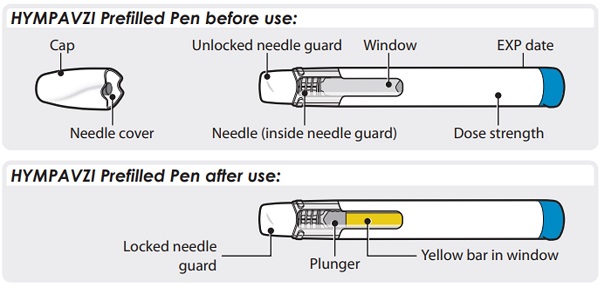
- Each HYMPAVZI Prefilled Pen is a Single-Dose Prefilled Pen (called “Pen” in this Instructions for Use). The HYMPAVZI Prefilled Pen contains 150 mg of HYMPAVZI for injection under the skin (subcutaneously).
- •
- Do not inject HYMPAVZI into a vein.
- •
- To help you remember when to inject HYMPAVZI, you can mark your calendar ahead of time. Call your healthcare provider if you or your caregiver have any questions about the right way to inject HYMPAVZI, or call the helpline at 1‑888‑496‑7289 (1‑888 HYMPAV‑Z).
- •
- Use HYMPAVZI exactly as prescribed by your healthcare provider.
- •
- HYMPAVZI is not made with natural rubber latex.
Storing HYMPAVZI
- •
- Store HYMPAVZI in a refrigerator at 36°F to 46°F (2°C to 8°C).
- •
- Store HYMPAVZI in the original carton to protect from light.
- •
- If needed, HYMPAVZI may be stored one time at room temperature, up to 86°F (30°C) in the original carton for up to 7 days. Do not return HYMPAVZI to the refrigerator after storing at room temperature.
- •
- Throw away (dispose of) HYMPAVZI that has been left out of the refrigerator for more than 7 days.
- •
- Do not freeze HYMPAVZI.
- •
- Do not shake HYMPAVZI.
- •
- Do not use past the expiration date (EXP) printed on the HYMPAVZI Prefilled Pen.
- •
- Keep HYMPAVZI and all medicines out of the reach of children.
Supplies Needed For HYMPAVZI Injection
Gather the following supplies on a clean flat surface:
Included in the carton:
- •
- 1 HYMPAVZI Prefilled Pen
Not included in the carton:
- •
- 1 alcohol swab
- •
- 1 cotton ball or gauze pad
- •
- 1 FDA-cleared sharps disposal container for Pen disposal (see “Step 10 – Disposal of Pen” and “Safe Pen Disposal” information section)
HYMPAVZI Prefilled Pen
Preparing to Inject HYMPAVZI
Step 1 – Getting Ready
- •
- Remove the Pen from its carton and keep out of direct sunlight.
- •
- Make sure the name HYMPAVZI appears on the carton and Pen label.
- •
- Check the Pen for any visible damage such as cracks or leaks.
- •
- Wash and dry your hands.
- •
- Do not remove the cap until you are ready to inject.
- •
- Throw away (dispose of) the Pen if it is damaged, or if the Pen or the carton containing the Pen has been dropped.
- •
- Do not use the Pen if:
- o
- it has been stored in direct light. Exposure to room light during dose preparation and injection is acceptable.
- o
- it has been frozen or thawed, or it has been out of the refrigerator for more than 7 days.
Note: For a more comfortable injection, allow the Pen to warm at room temperature up to 86°F (30°C) in the carton away from direct sunlight for about 15 to 30 minutes.
Do not use any other methods to warm up the Pen, such as warming the Pen in a microwave or hot water.
Step 2 – Check Expiration Date
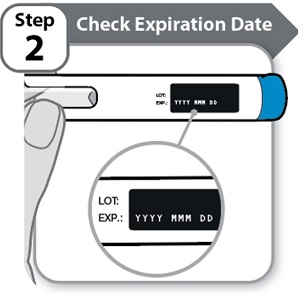
- •
- Check the expiration date (EXP) printed on the Pen label.
- •
- Do not use if the expiration date (EXP) has passed.
Step 3 – Check Medicine
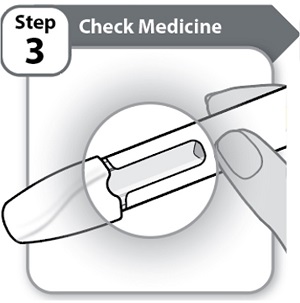
- •
- Look carefully at the medicine through the window on the Pen.
- o
- The medicine should be clear and colorless to light yellow.
- o
- Do not use the Pen if the medicine is cloudy, dark yellow, or contains flakes or particles.
Note: It is normal to see air bubbles in the window.
If you have any questions about the medicine, contact your healthcare provider.
Step 4 – Choose and Clean Your Injection Site
- •
- Choose an injection site on your stomach area (abdomen) or front of thigh unless a different site has been suggested by your healthcare provider. HYMPAVZI may also be injected into your buttocks by a healthcare provider or caregiver only. Keep at least 2 inches away from your belly button.
- •
- Change (rotate) the injection site each time you give yourself an injection of HYMPAVZI and away from any other medicine given under your skin. You may use the same area of your body but be sure to choose a different injection site in that area.
- •
- Clean the injection site with soap and water, or an alcohol swab.
- •
- Allow the site to air dry. Do not touch, fan, or blow on the cleaned injection site.
- •
- Do not inject HYMPAVZI into bony areas or areas on your skin that are bruised, red, sore (tender) or hard. Avoid injecting into areas with scars or stretch marks.
- •
- Do not inject HYMPAVZI into a vein.
- •
- Do not inject HYMPAVZI through your clothes.
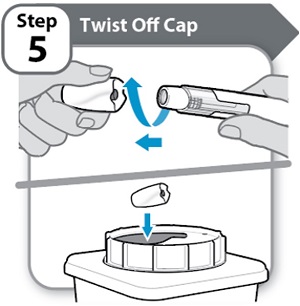
Step 5 – Twist Off Cap
- •
- Twist and pull off the cap.
- •
- Put the cap into an FDA-cleared sharps disposal container right away. You will not need it again.
Note:
- o
- It is normal to see a few drops of medicine at the needle tip.
- o
- The needle cover will stay inside the cap after cap removal.
Caution: Handle the Pen with care as it contains a needle.
Do not put or press your hand over the needle guard. Doing so may cause a needle injury.
Injecting HYMPAVZI
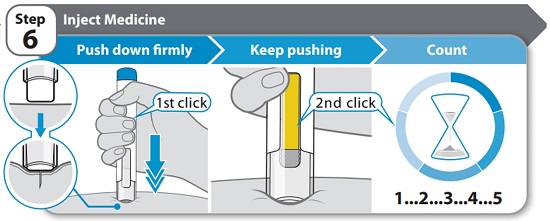
Step 6 – Inject Medicine
- •
- Hold the Pen straight (at 90° angle) against your clean skin so you can see the window.
- •
- Push the Pen down firmly straight against your skin and keep pushing until the injection is complete. You will hear the 1st click when the injection starts.
- •
- Keep pushing the Pen firmly against your skin while the yellow bar moves across the window. You will hear a 2nd click when the injection is almost complete.
- •
- Count slowly to 5 after you hear the 2nd click to make sure you get a full dose.
Do not remove the Pen from your skin until you have counted slowly to 5 after you hear the 2nd click and until the yellow marker completely fills the window.
Note: The needle goes into your skin as you push the Pen down. Your healthcare provider may suggest gently pinching your skin while you inject.
Note: If you do not hear a click when pushing the Pen against your skin, try pushing down harder. If you still cannot start the injection, get a new HYMPAVZI Prefilled Pen.
Caution: If you change your mind where to inject after inserting the needle into your skin, you will need to throw away (dispose of) the Pen and get a new HYMPAVZI Prefilled Pen.
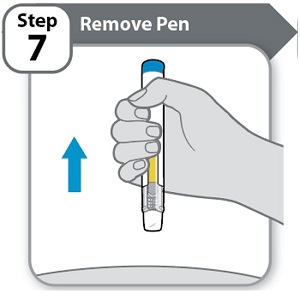
Step 7 – Remove Pen
- •
- Remove the Pen from your skin.
- o
- If you see a small drop of medicine on your skin, wait a little longer before removing the Pen when you give your next injection.
Note: After you remove the Pen from your skin, the needle guard will automatically cover the needle and lock in place.
The Pen cannot be reused.
Step 8 – Check Window
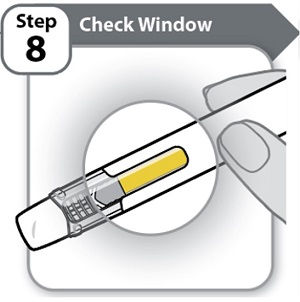
- •
- Check the window to make sure all the medicine has been injected.
If the yellow bar is not in the position shown, this means you have not received a full dose. Call your healthcare provider for help.
Do not inject another dose.
Step 9 – After Care

- •
- Press lightly on the injection site for a few seconds with a clean cotton ball or gauze pad if you see a drop of blood.
- •
- Do not rub the area.
Note: If bleeding does not stop, contact your healthcare provider.
Note: If your prescribed dose requires 2 injections of HYMPAVZI, repeat steps 1-9. Change (rotate) the injection site each time you give yourself an injection of HYMPAVZI. You may use the same area of your body but be sure to choose a different injection site in that area.
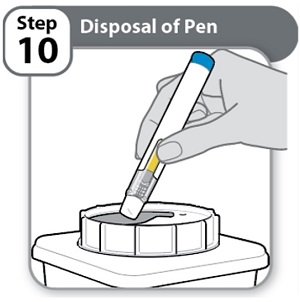
- •
- Put the used Pen in an FDA-cleared sharps disposal container right away after use.
- •
- Do not throw away (dispose of) Pens in the household trash.
Note: If you do not have an FDA-cleared sharps disposal container, please see the “Safe Pen Disposal” information section.
- •
- Always throw away (dispose of) Pens in a sharps disposal container. Do not dispose of Pens in the household trash.
- •
- If you do not have an FDA-cleared sharps disposal container, you may use a household container that:
- o
- is made of heavy-duty plastic,
- o
- can be closed with a tight-fitting, puncture-resistant lid, without sharps being able to come out,
- o
- is upright and stable during use,
- o
- is leak-resistant, and
- o
- is properly labeled to warn of hazardous waste inside the container.
- •
- When your sharps disposal container is almost full, you will need to follow your community guidelines for the right way to throw away (dispose of) your sharps disposal container. There may be state or local laws about how you should throw away used needles and Pens. For more information about safe sharps disposal, and for specific information about safe sharps disposal for the state you live in, go to the FDA’s website at: http://www.fda.gov/safesharpsdisposal.
- •
- Do not recycle your used sharps disposal container.

US License No. 2001
Distributed by
Pfizer Labs
Division of Pfizer Inc.
New York, NY 10001
LAB-1577-3.0
For more information, go to www.pfizer.com or call 1-800-438-1985.
This Instructions for Use has been approved by the U.S. Food and Drug Administration. Revised: 6/2026
INSTRUCTIONS FOR USE
HYMPAVZI® (him-PAV-zee)
(marstacimab-hncq)
injection, for subcutaneous use
75 mg single-dose prefilled syringe
This Instructions for Use contains information on how to inject HYMPAVZI.
Read this Instructions for Use carefully before using HYMPAVZI Prefilled Syringe and each time there is a refill prescription as there may be new information.
This HYMPAVZI Prefilled Syringe is for use in children 6 to less than 12 years of age and should be given by an adult caregiver only.
Your child’s healthcare provider should show a caregiver how to prepare and inject HYMPAVZI before they use it for the first time. Do not inject anyone until you have been shown how to inject HYMPAVZI.
Important Information You Need to Know Before Injecting HYMPAVZI
- •
- Each HYMPAVZI Prefilled Syringe is a Single-Dose Prefilled Syringe (called “Syringe” in this Instructions for Use). The HYMPAVZI Prefilled Syringe contains 75 mg of HYMPAVZI for injection under the skin (subcutaneously).
- •
- Do not inject HYMPAVZI into a vein.
- •
- To help remember when to inject HYMPAVZI, mark a calendar ahead of time. Call the healthcare provider if you have any questions about the right way to inject HYMPAVZI, or call the helpline at 1-888-496-7289 (1-888 HYMPAV-Z).
- •
- Use HYMPAVZI exactly as prescribed by the healthcare provider.
- •
- HYMPAVZI is not made with natural rubber latex.
Storing HYMPAVZI
- •
- Store HYMPAVZI in a refrigerator at 36°F to 46°F (2°C to 8°C).
- •
- Store HYMPAVZI in the original carton to protect from light.
- •
- If needed, HYMPAVZI may be stored one time at room temperature, up to 86°F (30°C) in the original carton for up to 7 days. Do not return HYMPAVZI to the refrigerator after storing at room temperature.
- •
- Throw away (dispose of) HYMPAVZI that has been left out of the refrigerator for more than 7 days.
- •
- Do not freeze HYMPAVZI.
- •
- Do not shake HYMPAVZI.
- •
- Do not use past the expiration date (Exp) printed on the HYMPAVZI Prefilled Syringe.
- •
- Keep HYMPAVZI and all medicines out of the reach of children.
Supplies Needed For HYMPAVZI Injection
Gather the following supplies on a clean flat surface:
Included in the carton:
- •
- 1 HYMPAVZI Prefilled Syringe
Not included in the carton:
- •
- 1 alcohol swab
- •
- 1 cotton ball or gauze pad
- •
- 1 FDA-cleared sharps disposal container for Syringe disposal (see “Step 11 – Disposal of Syringe” and “Safe Syringe Disposal” information section)
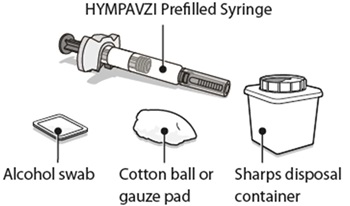
HYMPAVZI Prefilled Syringe
Always hold HYMPAVZI Prefilled Syringe by the barrel to prevent damage.
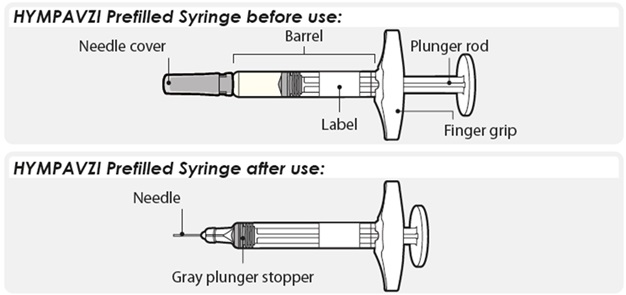
Preparing to Inject HYMPAVZI
Step 1 – Getting Ready
- •
- Remove the Syringe from its carton and keep out of direct sunlight.
- •
- Make sure the name HYMPAVZI appears on the carton and Syringe label.
- •
- Check the Syringe for any visible damage such as cracks or leaks.
- •
- Wash and dry your hands.
- •
- Do not remove the needle cover until you are ready to inject.
- •
- Throw away (dispose of) the Syringe if it is damaged, or if the Syringe or the carton containing the Syringe has been dropped.
- •
- Do not use the Syringe if:
- o
- it has been stored in direct light. Exposure to room light during dose preparation and injection is acceptable.
- o
- it has been frozen or thawed, or it has been out of the refrigerator for more than 7 days.
Note: For a more comfortable injection, allow the Syringe to warm at room temperature up to 86°F (30°C) in the carton away from direct sunlight for about 15 to 30 minutes.
Do not use any other methods to warm up the Syringe, such as warming the Syringe in a microwave or hot water.
Step 2 – Check Expiration Date

- •
- Check the expiration date (Exp) printed on the Syringe label.
- •
- Do not use if the expiration date (Exp) has passed.
Step 3 – Check Medicine

- •
- Gently tilt the Syringe back and forth.
- •
- Look carefully at the medicine in the Syringe.
- o
- The medicine should be clear and colorless to light yellow.
- o
- Do not use the Syringe if the medicine is cloudy, dark yellow, or contains flakes or particles.
Note: It is normal to see air bubbles in the Syringe.
If you have any questions about the medicine, contact the healthcare provider.
Step 4 – Choose and Clean the Injection Site
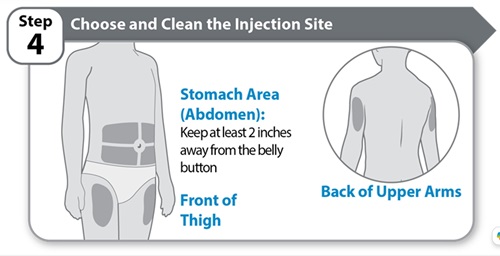
- •
- Choose an injection site on the stomach area (abdomen), front of thigh, or back of upper arms, unless a different site has been suggested by the healthcare provider. Keep at least 2 inches away from the belly button.
- •
- Change (rotate) the injection site each time you give an injection of HYMPAVZI and away from any other medicine given under the skin. The same area of the body may be used but be sure to choose a different injection site in that area.
- •
- Clean the injection site with soap and water, or an alcohol swab.
- •
- Allow the site to air dry. Do not touch, fan, or blow on the cleaned injection site.
- •
- Do not inject HYMPAVZI into bony areas or areas on the skin that are bruised, red, sore (tender) or hard. Avoid injecting into areas with scars or stretch marks.
- •
- Do not inject HYMPAVZI into a vein.
- •
- Do not inject HYMPAVZI through clothes.
Step 5 – Remove Cover

- •
- Hold the Syringe by the barrel.
- •
- Pull the needle cover straight off carefully.
- •
- Put the needle cover into an FDA-cleared sharps disposal container right away. You will not need it again.
- •
- Do not touch the needle or let it touch any surfaces.
Note: It is normal to see a few drops of medicine at the needle tip.
Caution: Handle the Syringe with care to avoid an accidental needle injury.
Injecting HYMPAVZI
Step 6 – Insert Needle
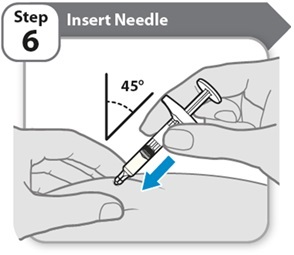
- •
- Pinch cleaned skin between your thumb and fingers to create a firm surface.
- •
- Fully insert the needle into the skin at a 45° angle, as shown. Do not hold or push on the plunger while inserting the needle.
Keep the skin pinched throughout the injection.
Caution: If you change your mind where to inject after inserting the needle into the skin, you will need to throw away (dispose of) the Syringe and get a new HYMPAVZI Prefilled Syringe.
Step 7 – Inject Medicine
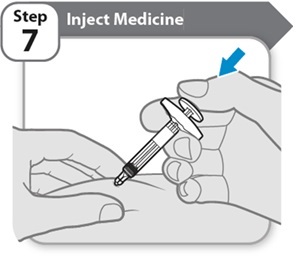
- •
- Slowly inject all of HYMPAVZI by gently pushing the plunger rod all the way down, until the barrel is empty.
Step 8 – Remove Needle
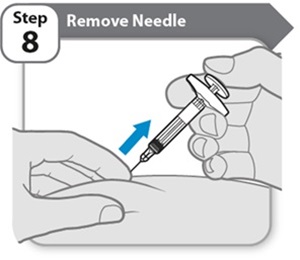
- •
- Pull the needle and Syringe out of the skin at the same angle as inserted.
Note: If you see a small drop of medicine on the skin, wait a little longer before removing the needle when you give the next injection.
Step 9 – Check Syringe

- •
- Check the Syringe to make sure the gray plunger stopper is in the position shown.
If the gray plunger stopper is not in the position shown, this means the full dose was not given. Call the healthcare provider for help.
Never re-insert the needle.
Do not inject another dose.
Step 10 – After Care

- •
- Press lightly on the injection site for a few seconds with a clean cotton ball or gauze pad if you see a drop of blood.
- •
- Do not rub the area.
Note: If bleeding does not stop, contact the healthcare provider.
Note: If the prescribed dose requires 2 injections of HYMPAVZI, repeat steps 1-10. Change (rotate) the injection site each time you give an injection of HYMPAVZI. You may use the same area of the body but be sure to choose a different injection site in that area.
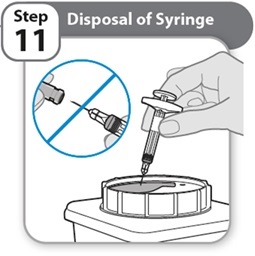
- •
- Put the used Syringe in an FDA-cleared sharps disposal container right away after use.
Never re-cap the needle.
- •
- Do not throw away (dispose of) Syringes in the household trash.
Note: If you do not have an FDA-cleared sharps disposal container, please see the “Safe Syringe Disposal” information section.
- •
- Always throw away (dispose of) Syringes in a sharps disposal container. Do not dispose of Syringes in the household trash.
- •
- If you do not have an FDA-cleared sharps disposal container, you may use a household container that:
- o
- is made of heavy-duty plastic,
- o
- can be closed with a tight-fitting, puncture-resistant lid, without sharps being able to come out,
- o
- is upright and stable during use,
- o
- is leak-resistant, and
- o
- is properly labeled to warn of hazardous waste inside the container.
- •
- When your sharps disposal container is almost full, you will need to follow your community guidelines for the right way to throw away (dispose of) your sharps disposal container. There may be state or local laws about how you should throw away used needles and syringes. For more information about safe sharps disposal, and for specific information about safe sharps disposal for the state you live in, go to the FDA’s website at: http://www.fda.gov/safesharpsdisposal.
- •
- Do not recycle your used sharps disposal container.

US License No. 2001
Distributed by
Pfizer Labs
Division of Pfizer Inc.
New York, NY 10001
LAB-1626-1.0
For more information, go to www.pfizer.com or call 1-800-438-1985.
This Instructions for Use has been approved by the U.S. Food and Drug Administration. Issued: 6/2026
INSTRUCTIONS FOR USE
HYMPAVZI® (him-PAV-zee)
(marstacimab-hncq)
injection, for subcutaneous use
75 mg single-dose prefilled pen
This Instructions for Use contains information on how to inject HYMPAVZI.
Read this Instructions for Use carefully before using HYMPAVZI Prefilled Pen and each time there is a refill prescription as there may be new information.
This HYMPAVZI Prefilled Pen is for use in children 6 to less than 12 years of age and should be given by an adult caregiver only.
Your child’s healthcare provider should show a caregiver how to prepare and inject HYMPAVZI before they use it for the first time. Do not inject anyone until you have been shown how to inject HYMPAVZI.
Important Information You Need to Know Before Injecting HYMPAVZI
- •
- Each HYMPAVZI Prefilled Pen is a Single-Dose Prefilled Pen (called “Pen” in this Instructions for Use). The HYMPAVZI Prefilled Pen contains 75 mg of HYMPAVZI for injection under the skin (subcutaneously).
- •
- Do not inject HYMPAVZI into a vein.
- •
- To help remember when to inject HYMPAVZI, mark a calendar ahead of time. Call the healthcare provider if you have any questions about the right way to inject HYMPAVZI, or call the helpline at 1‑888‑496‑7289 (1‑888 HYMPAV‑Z).
- •
- Use HYMPAVZI exactly as prescribed by the healthcare provider.
- •
- HYMPAVZI is not made with natural rubber latex.
Storing HYMPAVZI
- •
- Store HYMPAVZI in a refrigerator at 36°F to 46°F (2°C to 8°C).
- •
- Store HYMPAVZI in the original carton to protect from light.
- •
- If needed, HYMPAVZI may be stored one time at room temperature, up to 86°F (30°C) in the original carton for up to 7 days. Do not return HYMPAVZI to the refrigerator after storing at room temperature.
- •
- Throw away (dispose of) HYMPAVZI that has been left out of the refrigerator for more than 7 days.
- •
- Do not freeze HYMPAVZI.
- •
- Do not shake HYMPAVZI.
- •
- Do not use past the expiration date (EXP) printed on the HYMPAVZI Prefilled Pen.
- •
- Keep HYMPAVZI and all medicines out of the reach of children.
Supplies Needed For HYMPAVZI Injection
Gather the following supplies on a clean flat surface:
Included in the carton:
- •
- 1 HYMPAVZI Prefilled Pen
Not included in the carton:
- •
- 1 alcohol swab
- •
- 1 cotton ball or gauze pad
- •
- 1 FDA-cleared sharps disposal container for Pen disposal (see “Step 10 – Disposal of Pen” and “Safe Pen Disposal” information section)
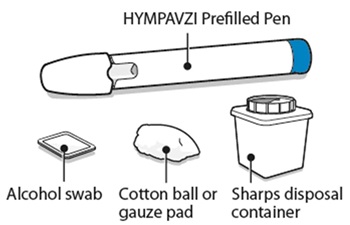
HYMPAVZI Prefilled Pen
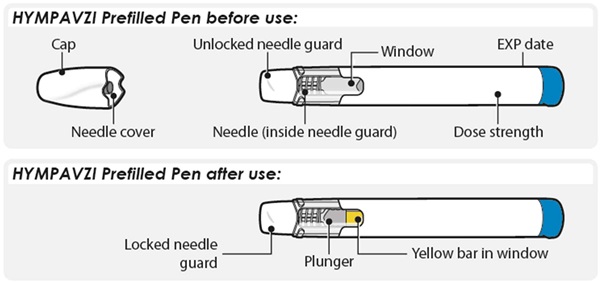
Preparing to Inject HYMPAVZI
Step 1 – Getting Ready
- •
- Remove the Pen from its carton and keep out of direct sunlight.
- •
- Make sure the name HYMPAVZI appears on the carton and Pen label.
- •
- Check the Pen for any visible damage such as cracks or leaks.
- •
- Wash and dry your hands.
- •
- Do not remove the cap until you are ready to inject.
- •
- Throw away (dispose of) the Pen if it is damaged, or if the Pen or the carton containing the Pen has been dropped.
- •
- Do not use the Pen if:
- o
- it has been stored in direct light. Exposure to room light during dose preparation and injection is acceptable.
- o
- it has been frozen or thawed, or it has been out of the refrigerator for more than 7 days.
Note: For a more comfortable injection, allow the Pen to warm at room temperature up to 86°F (30°C) in the carton away from direct sunlight for about 15 to 30 minutes.
Do not use any other methods to warm up the Pen, such as warming the Pen in a microwave or hot water.
Step 2 – Check Expiration Date

- •
- Check the expiration date (EXP) printed on the Pen label.
- •
- Do not use if the expiration date (EXP) has passed.
Step 3 – Check Medicine

- •
- Look carefully at the medicine through the window on the Pen.
- o
- The medicine should be clear and colorless to light yellow.
- o
- Do not use the Pen if the medicine is cloudy, dark yellow, or contains flakes or particles.
Note: It is normal to see air bubbles in the window.
If you have any questions about the medicine, contact the healthcare provider.
Step 4 – Choose and Clean the Injection Site
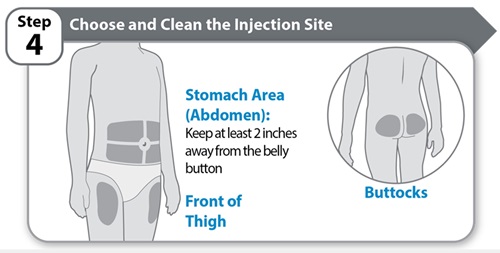
- •
- Choose an injection site on the stomach area (abdomen), front of thigh, or buttocks, unless a different site has been suggested by the healthcare provider. Keep at least 2 inches away from the belly button.
- •
- Change (rotate) the injection site each time you give an injection of HYMPAVZI and away from any other medicine given under the skin. The same area of the body may be used but be sure to choose a different injection site in that area.
- •
- Clean the injection site with soap and water, or an alcohol swab.
- •
- Allow the site to air dry. Do not touch, fan, or blow on the cleaned injection site.
- •
- Do not inject HYMPAVZI into bony areas or areas on the skin that are bruised, red, sore (tender) or hard. Avoid injecting into areas with scars or stretch marks.
- •
- Do not inject HYMPAVZI into a vein.
- •
- Do not inject HYMPAVZI through clothes.
Step 5 – Twist Off Cap
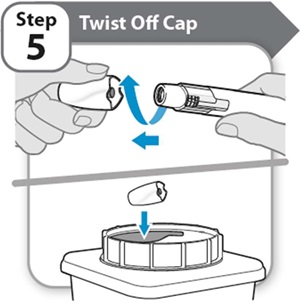
- •
- Twist and pull off the cap.
- •
- Put the cap into an FDA-cleared sharps disposal container right away. You will not need it again.
Note:
- o
- It is normal to see a few drops of medicine at the needle tip.
- o
- The needle cover will stay inside the cap after cap removal.
Caution: Handle the Pen with care as it contains a needle.
Do not put or press your hand over the needle guard. Doing so may cause a needle injury.
Injecting HYMPAVZI
Step 6 – Inject Medicine
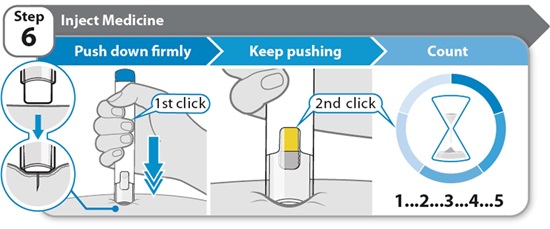
- •
- Hold the Pen straight (at 90° angle) against the clean skin so you can see the window.
- •
- Push the Pen down firmly straight against the skin and keep pushing until the injection is complete. You will hear the 1st click when the injection starts.
- •
- Keep pushing the Pen firmly against the skin while the yellow bar moves across the window. You will hear a 2nd click when the injection is almost complete.
- •
- Count slowly to 5 after you hear the 2nd click to make sure the full dose is given.
Do not remove the Pen from the skin until you have counted slowly to 5 after you hear the 2nd click and until the yellow marker completely fills the window.
Note: The needle goes into the skin as you push the Pen down. The healthcare provider may suggest gently pinching the skin while you inject.
Note: If you do not hear a click when pushing the Pen against the skin, try pushing down harder. If you still cannot start the injection, get a new HYMPAVZI Prefilled Pen.
Caution: If you change your mind where to inject after inserting the needle into the skin, you will need to throw away (dispose of) the Pen and get a new HYMPAVZI Prefilled Pen.
Step 7 – Remove Pen
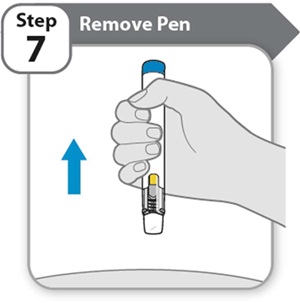
- •
- Remove the Pen from the skin.
- o
- If you see a small drop of medicine on the skin, wait a little longer before removing the Pen when you give the next injection.
Note: After removing the Pen from the skin, the needle guard will automatically cover the needle and lock in place.
The Pen cannot be reused.
Step 8 – Check Window
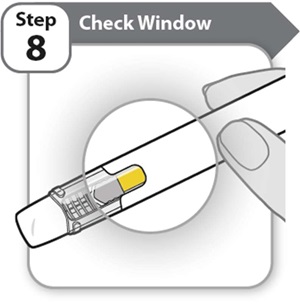
- •
- Check the window to make sure all the medicine has been injected.
If the yellow bar is not in the position shown, this means the full dose was not given. Call the healthcare provider for help.
Do not inject another dose.
Step 9 – After Care

- •
- Press lightly on the injection site for a few seconds with a clean cotton ball or gauze pad if you see a drop of blood.
- •
- Do not rub the area.
Note: If bleeding does not stop, contact the healthcare provider.
Note: If the prescribed dose requires 2 injections of HYMPAVZI, repeat steps 1-9. Change (rotate) the injection site each time you give an injection of HYMPAVZI. You may use the same area of the body but be sure to choose a different injection site in that area.
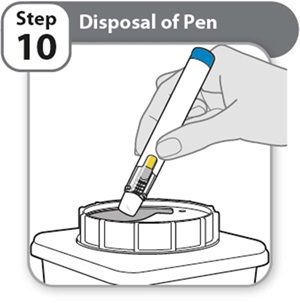
- •
- Put the used Pen in an FDA-cleared sharps disposal container right away after use.
- •
- Do not throw away (dispose of) Pens in the household trash.
Note: If you do not have an FDA-cleared sharps disposal container, please see the “Safe Pen Disposal” information section.
- •
- Always throw away (dispose of) Pens in a sharps disposal container. Do not dispose of Pens in the household trash.
- •
- If you do not have an FDA-cleared sharps disposal container, you may use a household container that:
- o
- is made of heavy-duty plastic,
- o
- can be closed with a tight-fitting, puncture-resistant lid, without sharps being able to come out,
- o
- is upright and stable during use,
- o
- is leak-resistant, and
- o
- is properly labeled to warn of hazardous waste inside the container.
- •
- When your sharps disposal container is almost full, you will need to follow your community guidelines for the right way to throw away (dispose of) your sharps disposal container. There may be state or local laws about how you should throw away used needles and Pens. For more information about safe sharps disposal, and for specific information about safe sharps disposal for the state you live in, go to the FDA’s website at: http://www.fda.gov/safesharpsdisposal.
- •
- Do not recycle your used sharps disposal container.

US License No. 2001
Distributed by
Pfizer Labs
Division of Pfizer Inc.
New York, NY 10001
LAB-1627-1.0
For more information, go to www.pfizer.com or call 1-800-438-1985.
This Instructions for Use has been approved by the U.S. Food and Drug Administration. Issued: 6/2026
MEDICATION GUIDE
MEDICATION GUIDE
| This Patient Information has been approved by the U.S. Food and Drug Administration. Revised: 6/2026 | |||
PATIENT INFORMATION HYMPAVZI® (him-PAV-zee) (marstacimab-hncq) injection, for subcutaneous use | |||
Important information:
| |||
What is HYMPAVZI? HYMPAVZI is a prescription medicine used regularly to prevent or reduce the frequency of bleeding episodes in adults and children 6 years of age and older with:
It is not known if HYMPAVZI is safe and effective in people receiving ongoing Immune Tolerance Induction (ITI). It is not known if HYMPAVZI is safe and effective in children younger than 6 years of age. | |||
Before using HYMPAVZI, tell your healthcare provider about all of your medical conditions, including if you:
Tell your healthcare provider about all the medicines you take, including prescription medicines, over‑the‑counter medicines, vitamins, and herbal supplements. Know the medicines you take. Keep a list of them to show your healthcare provider and pharmacist when you get a new medicine. | |||
How should I use HYMPAVZI? See the detailed “Instructions for Use” that comes with your HYMPAVZI for information on how to inject a dose of HYMPAVZI, and how to properly throw away (dispose of) used HYMPAVZI prefilled syringe or HYMPAVZI prefilled pen.
| |||
What are the possible side effects of HYMPAVZI? HYMPAVZI may cause serious side effects, including:
| |||
|
| ||
| |||
|
| ||
The most common side effects of HYMPAVZI include: | |||
|
| ||
These are not all of the possible side effects of HYMPAVZI. Call your doctor for medical advice about side effects. You may report side effects to FDA at 1-800-FDA-1088. | |||
How should I store HYMPAVZI?
Keep HYMPAVZI and all medicines out of the reach of children. | |||
General information about the safe and effective use of HYMPAVZI. Medicines are sometimes prescribed for purposes other than those listed in a Patient Information leaflet. Do not use HYMPAVZI for a condition for which it was not prescribed. Do not give HYMPAVZI to other people, even if they have the same symptoms that you have. It may harm them. You can ask your pharmacist or healthcare provider for information about HYMPAVZI that is written for health professionals. | |||
What are the ingredients in HYMPAVZI? Active ingredient: marstacimab‑hncq Inactive ingredients: edetate disodium, histidine, L-histidine monohydrochloride, polysorbate 80, sucrose, and water for injection | |||
This product's labeling may have been updated. For the most recent prescribing information, please visit www.pfizer.com.
| |||
Additional Resources
Chat online with Pfizer Medical Information regarding your inquiry on a Pfizer medicine or vaccine.
Speak with a Pfizer Medical Information Professional regarding your Pfizer medicine or vaccine inquiry.
Available 9AM-5PM ET Monday to Friday; excluding holidays.
Submit a medical question for a Pfizer medicine or a vaccine.
The submission will be reviewed during our standard business hours.
To report an adverse event related to a Pfizer product and you are not part of a clinical trial* for this medication, click the link below to submit your information:
Pfizer Safety Reporting Site
*If you are involved in a clinical trial for either product, adverse events should be reported to your coordinating study site.
If you cannot use the above website to report an adverse event related to a Pfizer medication, please call (800) 438-1985.
You may also contact the U.S. Food and Drug Administration (FDA) directly to report adverse events or product quality concerns either online at www.fda.gov/medwatch or by calling (800) 332-1088.