(medroxyprogesterone acetate)
14 CLINICAL STUDIES
14 CLINICAL STUDIES
14.1 Contraception Studies
In three open label clinical studies, depo-SubQ provera 104 (104 mg given every three months subcutaneously), was administered to healthy, sexually-active, nonpregnant women 18 to 49 years of age who desired long-term contraception. In these three studies, no pregnancies were detected among 2042 women treated with depo-subQ provera 104 for up to 1 year. In women less than 36 years of age (at baseline), the Pearl Index pregnancy rate in cycles in which no other contraceptive methods were used, was 0 pregnancies per 100 women-years of use (upper 95% CI = 0.25).
14.2 Endometriosis Studies
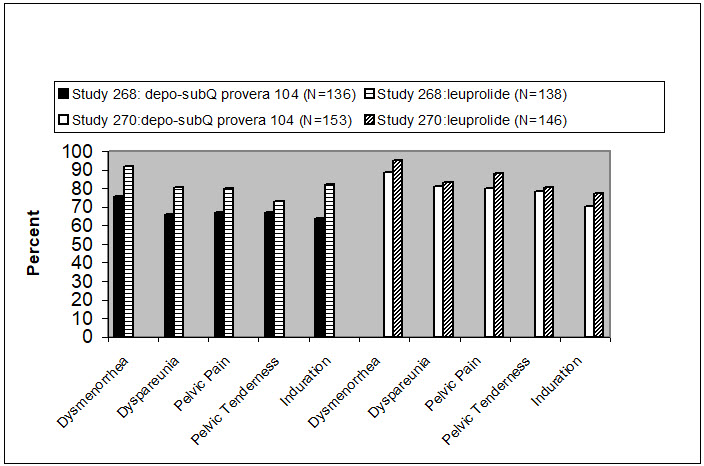
The efficacy of depo-subQ provera 104 in the reduction of endometriosis-associated pain in women with the signs and symptoms of endometriosis was demonstrated in two active comparator-controlled studies in pre-menopausal women 18 to 49 years of age with laparoscopically diagnosed endometriosis and persistent endometriosis pain symptoms (i.e., Studies 268 and 270). Each study assessed endometriosis-associated pain over 6 months of treatment and recurrence of symptoms for 12-months post treatment.
Subjects were treated for six months with depo-subQ provera 104 [104 mg given subcutaneously every 3 months (2 injections)] or leuprolide [11.25 mg given subcutaneously every 3 months (2 injections) or 3.75 mg given subcutaneously every month (6 injections)]. Study 268 was conducted in the U.S. and Canada and enrolled 274 subjects (136 subjects received depo-subQ provera 104 and 138 subjects received leuprolide). Study 270 was conducted in South America, Europe, and Asia, and enrolled 299 subjects (153 subjects received depo-subQ provera 104 and 146 subjects received leuprolide).
Reduction in endometriosis pain was evaluated using a modified Biberoglu and Behrman scale that consisted of three patient-reported symptoms (i.e., dysmenorrhea, dyspareunia, and pelvic pain not related to menses) and two signs assessed during pelvic examination (i.e., pelvic tenderness and induration). For each category, a favorable response was defined as improvement of at least 1 unit (severity was assessed on a scale of 0 to 3) relative to baseline score (Figure Q).
Additionally, scores from each of the five categories were combined into a composite score that was considered a global measurement of overall disease improvement. For subjects with baseline scores for each of the 5 categories, a mean decrease of 4 points relative to baseline was considered a clinically meaningful improvement. Across both studies, the mean changes in the composite score met the protocol-defined criterion for improvement for the depo-subQ provera 104 and leuprolide treatment groups.
In the clinical trials, treatment with depo-subQ provera 104 was limited to six months. Data on the persistence of benefit with longer treatment are not available.
14.3 Bone Mineral Density in Women Treated with Depo-medroxyprogesterone acetate for Contraception
In a study that compared changes in bone mineral density (BMD) in adult women using depo-subQ provera 104 or DMPA-IM for contraception, both treatments showed BMD reductions in the lumbar spine, total hip, and femoral neck. Mean percent changes in BMD in depo-subQ provera 104-treated women are shown in Table 3.
| Time on Treatment | Lumbar Spine | Total Hip | Femoral Neck |
|---|---|---|---|
| Mean % Change (95% CI) | Mean % Change (95% CI) | Mean % Change (95% CI) | |
1 year | -2.7 | -1.7 | -1.9 |
2 years | - 4.1 | -3.5 | -3.5 |
BMD Recovery Post-Treatment in Women
Given the similar effects on BMD from depo-subQ provera 104 and DMPA-IM described above, BMD recovery post-treatment is also expected to be similar. In a controlled clinical study that compared changes in BMD in adult women using DMPA-IM for contraception or no hormonal contraception, the 2-year post-treatment follow-up demonstrated incomplete recovery of BMD following the last injection of DMPA-IM. Table 4 shows the change in BMD in women after 5 years of treatment with DMPA-IM and in the control group, as well as the extent of BMD recovery in the subset of women for whom 2-year post-treatment data were available.
| Time in Study | Spine | Total Hip | Femoral Neck | |||
|---|---|---|---|---|---|---|
| DMPA-IM* | Control† | DMPA-IM* | Control† | DMPA-IM* | Control† | |
5 years | -5.38% | 0.43% | -5.16% | 0.19% | -6.12% | -0.27% |
7 years | -3.13% | 0.53% | -1.34% | 0.94% | -5.38% | -0.11% |
14.4 Bone Mineral Density Changes in Adolescent Females (12 to 18 years of age) Treated with DMPA-IM
The effect of DMPA-IM on BMD in adolescents is described below, and the effect of depo-subQ provera 104 on BMD in adolescents is expected to be similar. The impact of DMPA-IM use for up to 240 weeks (4.6 years) was evaluated in an open-label non-randomized clinical study in 389 adolescent females (12 to 18 years of age). Use of DMPA-IM was associated with a significant decline from baseline in BMD.
Partway through the trial, DMPA-IM administration was stopped (at 120 weeks). The mean number of injections per DMPA-IM user was 9.3. Table 5 summarizes the study findings. The decline in BMD at total hip and femoral neck was greater with longer duration of use. The mean decrease in BMD at 240 weeks was more pronounced at total hip (-6.4%) and femoral neck (-5.4%) compared to lumbar spine (-2.1%).
Adolescents in the untreated cohort had an increase in BMD during the period of growth following menarche. However, the two cohorts were not matched at baseline for age, gynecologic age, race, BMD, and other factors that influence the rate of acquisition of BMD.
| Duration of Treatment | DMPA-IM (150 mg) | Unmatched, Untreated Cohort | ||
|---|---|---|---|---|
| N | Mean % Change | N | Mean % Change | |
Total Hip BMD | ||||
Week 60 (1.2 years) | 113 | -2.75 | 166 | 1.22 |
Week 120 (2.3 years) | 73 | -5.40 | 109 | 2.19 |
Week 240 (4.6 years) | 28 | -6.40 | 84 | 1.71 |
Femoral Neck BMD | ||||
Week 60 | 113 | -2.96 | 166 | 1.75 |
Week 120 | 73 | -5.30 | 108 | 2.83 |
Week 240 | 28 | -5.40 | 84 | 1.94 |
Lumbar Spine BMD | ||||
Week 60 | 114 | -2.47 | 167 | 3.39 |
Week 120 | 73 | -2.74 | 109 | 5.28 |
Week 240 | 27 | -2.11 | 84 | 6.40 |
BMD Recovery Post-Treatment in Adolescents
Longer duration of treatment and smoking were associated with less recovery of BMD following the last injection of DMPA-IM. Table 6 shows the extent of recovery of BMD up to 60 months post-treatment for adolescents who received DMPA-IM for two years or less compared to more than two years. Post-treatment follow-up showed that, in adolescents treated for more than two years, only lumbar spine BMD recovered to baseline levels after treatment was discontinued. Adolescents treated with DMPA-IM for more than two years did not recover to their baseline BMD level at the femoral neck and total hip even up to 60 months post-treatment. Adolescents in the untreated cohort gained BMD throughout the trial period [see Warnings and Precautions (5.1)].
| Duration of Treatment (Months) | 2 Years or Less | More than 2 Years | ||
|---|---|---|---|---|
| N | Mean % Change from baseline | N | Mean % Change from baseline | |
Total Hip BMD | ||||
End of Treatment | 49 | -1.5% | 49 | -6.2% |
12 M post-treatment | 33 | -1.4% | 24 | -4.6% |
24 M post-treatment | 18 | 0.3% | 17 | -3.6% |
36 M post-treatment | 12 | 2.1% | 11 | -4.6% |
48 M post-treatment | 10 | 1.3% | 9 | -2.5% |
60 M post-treatment | 3 | 0.2% | 2 | -1.0% |
Femoral Neck BMD | ||||
End of Treatment | 49 | -1.6% | 49 | -5.8% |
12 M post-treatment | 33 | -1.4% | 24 | -4.3% |
24 M post-treatment | 18 | 0.5% | 17 | -3.8% |
36 M post-treatment | 12 | 1.2% | 11 | -3.8% |
48 M post-treatment | 10 | 2.0% | 9 | -1.7% |
60 M post-treatment | 3 | 1.0% | 2 | -1.9% |
Lumbar Spine BMD | ||||
End of Treatment | 49 | -0.9% | 49 | -3.5% |
12 M post-treatment | 33 | 0.4% | 23 | -1.1% |
24 M post-treatment | 18 | 2.6% | 17 | 1.9% |
36 M post-treatment | 12 | 2.4% | 11 | 0.6% |
48 M post-treatment | 10 | 6.5% | 9 | 3.5% |
60 M post-treatment | 3 | 6.2% | 2 | 5.7% |
14.5 Bone Fracture Incidence in Women Treated with Depo-medroxyprogesterone acetate for Contraception
A retrospective cohort study to assess the association between DMPA-IM injection and the incidence of bone fractures was conducted in 312,395 female contraceptive users in the UK. The incidence rates of fracture were compared between DMPA-IM users and contraceptive users who had no recorded use of DMPA-IM. The Incident Rate Ratio (IRR) for any fracture during the follow-up period (mean=5.5 years) was 1.41 (95% CI 1.35, 1.47). It is not known if this is due to DMPA-IM use or to other related lifestyle factors that have a bearing on fracture rate.
In the study, when cumulative exposure to DMPA-IM was calculated, the fracture rate in users who received fewer than 8 injections was higher than that in women who received 8 or more injections. However, it is not clear that cumulative exposure, which may include periods of intermittent use separated by periods of non-use, is a useful measure of risk, as compared to exposure measures based on continuous use.
There were very few osteoporotic fractures (fracture sites known to be related to low BMD) in the study overall, and the incidence of osteoporotic fractures was not found to be higher in DMPA-IM users compared to non-users.
Importantly, this study could not determine whether use of DMPA-IM has an effect on fracture rate later in life. Given the similar effects on BMD from depo-subQ provera 104 and DMPA-IM described above, bone fracture incidence may also be expected to be similar.
14.6 Bone Mineral Density in Women Treated with depo-SubQ provera 104 for Endometriosis
In two clinical studies of 573 adult women with endometriosis, the BMD effects of 6 months of depo-subQ provera 104 treatment (104 mg subcutaneously every 3 months) were compared to 6 months of leuprolide treatment (either 11.25 mg given subcutaneously every 3 months or 3.75 mg given subcutaneously every month). Subjects were then observed after treatment completion, for an additional 12 months. See Table 7 for the results.
| Time of BMD Measurement | Lumbar Spine | Total Hip | ||||||
|---|---|---|---|---|---|---|---|---|
| depo-subQ provera 104 | Leuprolide | depo-subQ provera 104 | Leuprolide | |||||
| N | Mean % Change | N | Mean % Change | N | Mean % Change | N | Mean % Change | |
Month 6 of treatment (End of Treatment) | 208 | -1.20 | 229 | -4.10 | 207 | -0.03 | 227 | -1.83 |
6 months post-treatment | 168 | -1.06 | 180 | -2.75 | 169 | -0.05 | 181 | -1.59 |
12 months post-treatment | 124 | -0.54 | 133 | -1.48 | 125 | 0.39 | 134 | -1.15 |
MEDICATION GUIDE
PATIENT INFORMATION
DEPO-SUBQ PROVERA 104®
(deh-poh' sub-cue' pro-ver-ah' one-oh-four)
(medroxyprogesterone acetate injectable suspension)
for subcutaneous use
WHAT IS THE MOST IMPORTANT INFORMATION I SHOULD KNOW ABOUT depo-subQ provera 104?
Use of depo-subQ provera 104 may cause you to lose calcium stored in your bones. The longer you use depo-subQ provera 104 the more calcium you are likely to lose. The calcium may not return completely once you stop using depo-subQ provera 104.
Loss of calcium may cause weak, porous bones (osteoporosis) that could increase the risk that your bones might break, especially after menopause. It is not known whether your risk of developing osteoporosis may be greater if you are a teenager when you start to use depo-subQ provera 104.
You should use depo-subQ provera 104 long-term (for example, more than 2 years) only if other methods of birth control or other treatments for endometriosis pain are not right for you.
Depo-subQ provera 104 does not protect you from HIV (AIDS) and other sexually transmitted infections (STIs).
WHAT IS depo-subQ provera 104?
Depo-subQ provera 104 is a drug for birth control. It also helps relieve pain related to endometriosis (en-do-ME-tree-OH-sis). Symptoms of endometriosis arise when cells normally inside your uterus grow outside the uterus. The cells respond to menstrual cycle hormones, and may cause painful periods, pelvic pain, and painful sex.
Depo-subQ provera 104 contains a hormone called medroxyprogesterone acetate (MPA). It is given as a shot (injection) every 3 months. Three months is the same as 12 to 14 weeks.
HOW WELL DOES depo-subQ provera 104 WORK FOR PREVENTING PREGNANCY?
When you use depo-subQ provera 104 correctly, the chance of getting pregnant is very low. In studies, no women became pregnant during the year they used depo-subQ provera 104 injection.
The list below estimates the chances of getting pregnant using different types of birth control. The numbers are based on typical use. Typical use includes people who use the method correctly and people who use the method incorrectly. The list shows the number of women out of 100 women who will likely get pregnant if they use the method for 1 year.
| Method | Typical Chance of Getting Pregnant in 1 year (Number of pregnancies in 100 women) |
|---|---|
Shot | Less than 1 |
Pill | 5 |
Condom alone (male) | 14 |
Withdrawal | 19 |
Diaphragm with spermicides | 20 |
Condom alone (female) | 21 |
Periodic abstinence | 25 |
Spermicides alone | 26 |
Vaginal sponge or Cervical cap with spermicide | 20 to 40 |
HOW WILL I GET depo-subQ provera 104?
Depo-subQ provera 104 is given as a shot just under the skin on your thigh or belly. You get it once every 3 months.
For Birth Control
First shot:
Your healthcare professional will want to be sure that you are not pregnant before you get your first shot. Normally, you get the shot by the 5th day from the START of your menstrual period. You get it whether or not you are still bleeding.
If you are breast-feeding, you may have your first shot as early as 6 weeks after you deliver your baby.
After the first shot:
It is very important to keep getting depo-subQ provera 104 every 3 months. If you wait more than 14 weeks between shots, you could become pregnant. Your healthcare professional must make sure you are not pregnant before you get your next shot.
When you get your shot, make an appointment for your next shot. Mark it on your calendar.
If you need a birth control method for more than two years, your healthcare professional may ask you to have a test of your bones or ask you to switch to another birth control method before continuing depo-subQ provera 104, especially if you have other risks for weak bones.
For Endometriosis
If you have regular periods, you will get depo-subQ provera 104 the same way as described above for birth control. If your periods have stopped or are not regular, your healthcare professional must test to make sure you are not pregnant before you get your first shot.
It is not recommended that you receive depo-subQ provera 104 for treatment of endometriosis for longer than 2 years. If your painful symptoms return after stopping treatment, your healthcare professional should ask you to have a test of your bones before restarting treatment.
WHAT IF I MISS A SHOT?
If you miss a shot, or wait longer than 14 weeks between shots, you could get pregnant. The longer you wait, the greater the risk of getting pregnant.
Talk with your healthcare professional to find out when to restart depo-subQ provera 104. You should be tested to be sure you are not pregnant.
Use another kind of non-hormonal birth control, such as condoms, until you start depo-subQ provera 104 again.
DO NOT TAKE depo-subQ provera 104 IF YOU…
- •
- Have any unexplained vaginal bleeding
- •
- Have or have ever had breast cancer or think you have breast cancer
- •
- Ever had serious blood clots, such as blood clots in your legs (deep venous thrombophlebitis), lungs (pulmonary embolism), heart (heart attack), or head (stroke)
- •
- Have liver disease
- •
- Are allergic to anything in depo-subQ provera 104. There is a list of what is in depo-subQ provera 104 at the end of this leaflet.
BEFORE TAKING depo-subQ provera 104
Your healthcare professional may do a physical examination and check your blood and urine.
Tell your healthcare professional about all your medical conditions.
Most importantly, tell your healthcare professional if you:
- •
- Are pregnant or might be pregnant. You should not get depo-subQ provera 104 if you are pregnant.
- •
- Plan to become pregnant in the next year. After you stop getting depo-subQ provera 104, it takes time for your body to be able to get pregnant. It can be as early as 1 week after the last shot wears off. Most likely it will take up to 1 year or longer for you to get pregnant.
- •
- Have or have ever had breast cancer, or think you have breast cancer
- •
- Have breast cancer in your family
- •
- Have an abnormal mammogram (breast X-ray), lumps in your breast, or bleeding from your nipples
- •
- Have or have ever had a type of usually benign brain tumor called a meningioma
- •
- Have irregular, light, or heavy menstrual periods
- •
- Have or had any of the following medical problems:
- o
- Kidney problems
- o
- High blood pressure
- o
- Migraine headaches
- o
- Asthma
- o
- Seizures
- o
- Diabetes, or if it runs in your family
- o
- Depression
- o
- Heart attack, stroke, or blood clots
- o
- Bone disease
- o
- Anorexia nervosa (an eating disorder)
- o
- A strong family history of osteoporosis
- o
- Use of a drug that can lower the amount of calcium in bones (drugs for epilepsy or steroids)
- o
- Drinking a lot of alcohol or smoking a lot
It is important to see your healthcare professional regularly if you have any of these conditions.
Some medicines may make depo-subQ provera 104 less effective at preventing pregnancy, including those listed below:
- •
- Bosentan (used to treat pulmonary arterial hypertension)
- •
- Efavirenz, etravirine (HIV medicines)
- •
- Modafinil (used to improve wakefulness)
- •
- Mitotane (used to treat adrenal cortical carcinoma)
- •
- Phenytoin, carbamazepine, phenobarbital (used to treat seizures)
- •
- Rifampin (an antibiotic)
- •
- St. John's Wort (herbal medicinal product)
Tell your healthcare professional about all the medicines you take. This includes prescription and over-the-counter medicines, vitamins, and herbal products.
WHAT ELSE SHOULD I KNOW ABOUT TAKING depo-subQ provera 104?
Other Birth Control. If you can't take birth control pills or can't use a birth control patch or ring, you may be able to use depo-subQ provera 104. Ask your healthcare professional.
Pregnancy. When you take depo-subQ provera 104 every 3 months, your chance of getting pregnant is very low. You could miss a period or have a light period and not be pregnant. If you miss 1 or 2 periods and think you might be pregnant, see your healthcare professional as soon as possible.
You should not use depo-subQ provera 104 if you are pregnant. However, depo-subQ provera 104 taken by accident during pregnancy does not seem to cause birth defects.
Pregnancy in your fallopian tubes (Ectopic Pregnancy). If you have severe pain low in your belly, tell your healthcare professional right away. Infrequently, a baby may start to grow outside the uterus, most often in the tubes.
Nursing a baby. Wait at least 6 weeks after your baby is born to start depo-subQ provera 104. You can use depo-subQ provera 104 if you are nursing.
It does not lower the amount of milk you can make.
It can pass through breast milk into your baby, but it is not harmful.
Blood or urine tests. Depo-subQ provera 104 may affect blood or urine test results. Tell your healthcare professional you are taking depo-subQ provera 104 if you are going to have blood or urine tests.
Liver problems. Your healthcare professional may stop depo-subQ provera 104 if you have liver problems. Some signs of liver problems are yellow skin or eyes, feeling like you have the flu, feeling more tired than usual, and itching. Tell your healthcare professional if you have these symptoms.
WHAT ARE THE MOST SERIOUS RISKS OF depo-subQ provera 104?
Losing calcium from your bones. Depo-subQ provera 104 use may decrease the amount of calcium in your bones. The longer you use depo-subQ provera 104, the more calcium you are likely to lose. This increases the risk of your bones weakening if you use depo-subQ provera 104 continuously for a long time (for example, if you use depo-subQ provera 104 for more than 2 years). The loss of calcium may increase your risk of osteoporosis and broken bones, particularly after your menopause.
Calcium is generally added to the bones during teenage years. The decrease of calcium in your bones is of most concern if you are a teenager or have the following risk factors:
- •
- Bone disease
- •
- Anorexia nervosa (an eating disorder)
- •
- A strong family history of osteoporosis
- •
- Using a drug that can lower the amount of calcium in bones (drugs for epilepsy or steroids), or
- •
- Drinking a lot of alcohol or smoking a lot
If you need a birth control method for more than 2 years, your healthcare professional may ask you to have a test of your bones or ask you to switch to another birth control method before continuing depo-subQ provera 104, especially if you have other risks for weak bones. When depo-subQ provera 104 is stopped, the calcium in your bones begins to come back. The lost calcium may not return completely once you stop using depo-subQ provera 104.
Abnormal or very heavy bleeding. If you start having very heavy or very long periods, tell your healthcare professional.
Allergic reaction. Allergic reactions to depo-subQ provera 104 have been reported. If you have hives, problems breathing, swelling of the face, mouth, tongue, or neck, or just do not feel right after your shot, call your healthcare professional or go to the Emergency Room right away.
Serious blood clots. Call your healthcare professional immediately if you:
- •
- Have sharp chest pain, cough blood, or suddenly have trouble breathing
- •
- Have a sudden severe headache with vomiting, blindness or trouble talking, weakness, or numbness in an arm or leg, or get dizzy or faint
- •
- Have swelling or severe pain in your leg
Depression. If you suffer from depression or have a history of depression, inform your healthcare professional if you notice any worsening of your depression while taking depo-subQ provera 104.
Meningioma (a type of usually benign brain tumor). Possible increased risk for growth of a meningioma, primarily when the product is used for a long time.
WHAT ARE COMMON SIDE EFFECTS OF depo-subQ provera 104?
The most common side effects are:
- •
- Changes in your monthly periods. You may not know when you will bleed, your periods may not be regular, you may have heavy bleeding, or you may have spotting. You may have more days of bleeding during the first 2 or 3 months after you start depo-subQ provera 104. Over time, you may have less and less bleeding. Many women stop having periods by the end of 1 year. Your periods will come back eventually after you stop using depo-subQ provera 104.
- •
- Headache.
- •
- Weight gain. In studies, women gained an average of 3 to 4 pounds during the first year they used depo-subQ provera 104. After 2 years of using depo-subQ provera 104, women gained an average of 7 to 8 pounds. Some women gained more, some gained less, some lost, and some stayed the same. Weight changes beyond 2 years of use with depo-subQ provera 104 have not been studied. Women who used a similar birth control product for 5 years gained on average 5 pounds more than women who did not use a hormone contraceptive product.
- •
- Skin reaction where you got the shot. Lumps, skin dimpling, or pain may occur. Scarring and discoloration are uncommon, but may happen. If there is swelling or your skin gets hot, has pus or looks bruised 1 or more days after your shot, call your healthcare professional.
Women using depo-subQ provera 104 for birth control or endometriosis had these less common side effects: Vaginal inflammation, vaginal thrush, abdominal pain, urinary tract infections, acne, depression, less sex drive, nausea, back pain, breast pain/tenderness, fatigue, anxiety, being irritable, dizziness, hot flushes and fluid retention.
If you feel you are having other side effects, talk with your healthcare professional.
DOES depo-subQ provera 104 CAUSE CANCER?
There have been several studies of women who use birth control like depo-subQ provera 104.
- •
- Women who use depo-subQ provera 104 may have a slightly increased risk of breast cancer compared to non-users.
- •
- The risk of cancer of the ovary, liver, or cervix did not change.
WHAT IF I WANT TO BECOME PREGNANT?
Plan ahead. The effect of depo-subQ provera 104 can last for a long time after you stop getting shots. Although you may be able to get pregnant quickly, it is more likely to take a year or longer after your last shot before you get pregnant.
It's best to see your healthcare professional for a pre-pregnancy check-up. Your healthcare professional may also tell you to take a vitamin called folic acid every day if you are planning to become pregnant.
GENERAL ADVICE ABOUT depo-subQ provera 104
For more information about depo-subQ provera 104, ask your healthcare professional or pharmacist.
WHAT IS IN depo-subQ provera 104?
Active ingredient: medroxyprogesterone acetate.
Inactive ingredients: methylparaben, propylparaben, sodium chloride, polyethylene glycol, polysorbate 80, monobasic sodium phosphate∙H2O, dibasic sodium phosphate∙12H2O, methionine, povidone, water for shot. When necessary, the pH is adjusted with sodium hydroxide or hydrochloric acid, or both.
This product's labeling may have been updated. For the most recent prescribing information, please visit www.pfizer.com.

LAB-0298-12.0
Revised December 2025
Additional Resources
Chat online with Pfizer Medical Information regarding your inquiry on a Pfizer medicine or vaccine.
Speak with a Pfizer Medical Information Professional regarding your Pfizer medicine or vaccine inquiry.
Available 9AM-5PM ET Monday to Friday; excluding holidays.
Submit a medical question for a Pfizer medicine or a vaccine.
The submission will be reviewed during our standard business hours.
To report an adverse event related to a Pfizer product and you are not part of a clinical trial* for this medication, click the link below to submit your information:
Pfizer Safety Reporting Site
*If you are involved in a clinical trial for either product, adverse events should be reported to your coordinating study site.
If you cannot use the above website to report an adverse event related to a Pfizer medication, please call (800) 438-1985.
You may also contact the U.S. Food and Drug Administration (FDA) directly to report adverse events or product quality concerns either online at www.fda.gov/medwatch or by calling (800) 332-1088.