(varenicline tartrate)
14 CLINICAL STUDIES
14 CLINICAL STUDIES
The efficacy of CHANTIX in smoking cessation was demonstrated in six clinical trials in which a total of 3659 chronic cigarette smokers (≥10 cigarettes per day) were treated with CHANTIX. In all clinical studies, abstinence from smoking was determined by patient self-report and verified by measurement of exhaled carbon monoxide (CO≤10 ppm) at weekly visits. Among the CHANTIX-treated patients enrolled in these studies, the completion rate was 65%. Except for the dose-ranging study (Study 1) and the maintenance of abstinence study (Study 6), patients were treated for 12 weeks and then were followed for 40 weeks post-treatment. Most patients enrolled in these trials were white (79–96%). All studies enrolled almost equal numbers of men and women. The average age of patients in these studies was 43 years. Patients on average had smoked about 21 cigarettes per day for an average of approximately 25 years. Patients set a date to stop smoking (target quit date) with dosing starting 1 week before this date.
Seven additional studies evaluated the efficacy of CHANTIX in patients with cardiovascular disease, in patients with chronic obstructive pulmonary disease [see Clinical Studies (14.7)], in patients instructed to select their quit date within days 8 and 35 of treatment [see Clinical Studies (14.4)], patients with major depressive disorder [see Clinical Studies (14.9)], patients who had made a previous attempt to quit smoking with CHANTIX, and either did not succeed in quitting or relapsed after treatment [see Clinical Studies (14.6)], in patients without or with a history of psychiatric disorder enrolled in a postmarketing neuropsychiatric safety outcome trial [see Warnings and Precautions (5.1), Clinical Studies (14.10)], and in patients who were not able or willing to quit abruptly and were instructed to quit gradually [see Clinical studies (14.5)].
In all studies, patients were provided with an educational booklet on smoking cessation and received up to 10 minutes of smoking cessation counseling at each weekly treatment visit according to Agency for Healthcare Research and Quality guidelines.
14.1 Initiation of Abstinence
Study 1
This was a six-week dose-ranging study comparing CHANTIX to placebo. This study provided initial evidence that CHANTIX at a total dose of 1 mg per day or 2 mg per day was effective as an aid to smoking cessation.
Study 2
This study of 627 patients compared CHANTIX 1 mg per day and 2 mg per day with placebo. Patients were treated for 12 weeks (including one-week titration) and then were followed for 40 weeks post-treatment. CHANTIX was given in two divided doses daily. Each dose of CHANTIX was given in two different regimens, with and without initial dose-titration, to explore the effect of different dosing regimens on tolerability. For the titrated groups, dosage was titrated up over the course of one week, with full dosage achieved starting with the second week of dosing. The titrated and nontitrated groups were pooled for efficacy analysis.
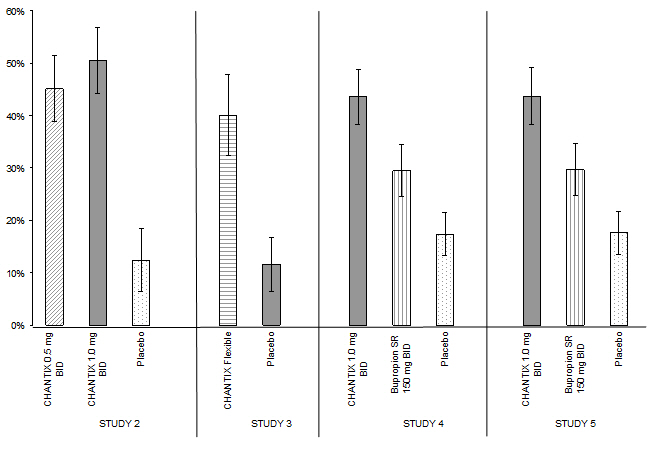
Forty-five percent of patients receiving CHANTIX 1 mg per day (0.5 mg twice daily) and 51% of patients receiving 2 mg per day (1 mg twice daily) had CO-confirmed continuous abstinence during weeks 9 through 12 compared to 12% of patients in the placebo group (Figure 1). In addition, 31% of the 1 mg per day group and 31% of the 2 mg per day group were continuously abstinent from one week after TQD through the end of treatment as compared to 8% of the placebo group.
Study 3
This flexible-dosing study of 312 patients examined the effect of a patient-directed dosing strategy of CHANTIX or placebo. After an initial one-week titration to a dose of 0.5 mg twice daily, patients could adjust their dosage as often as they wished between 0.5 mg once daily to 1 mg twice daily per day. Sixty-nine percent of patients titrated to the maximum allowable dose at any time during the study. For 44% of patients, the modal dose selected was 1 mg twice daily; for slightly over half of the study participants, the modal dose selected was 1 mg/day or less.
Of the patients treated with CHANTIX, 40% had CO-confirmed continuous abstinence during weeks 9 through 12 compared to 12% in the placebo group. In addition, 29% of the CHANTIX group were continuously abstinent from one week after TQD through the end of treatment as compared to 9% of the placebo group.
Study 4 and Study 5
These identical double-blind studies compared CHANTIX 2 mg per day, bupropion sustained-release (SR) 150 mg twice daily, and placebo. Patients were treated for 12 weeks and then were followed for 40 weeks post-treatment. The CHANTIX dosage of 1 mg twice daily was achieved using a titration of 0.5 mg once daily for the initial 3 days followed by 0.5 mg twice daily for the next 4 days. The bupropion SR dosage of 150 mg twice daily was achieved using a 3-day titration of 150 mg once daily. Study 4 enrolled 1022 patients and Study 5 enrolled 1023 patients. Patients inappropriate for bupropion treatment or patients who had previously used bupropion were excluded.
In Study 4, patients treated with CHANTIX had a superior rate of CO-confirmed abstinence during weeks 9 through 12 (44%) compared to patients treated with bupropion SR (30%) or placebo (17%). The bupropion SR quit rate was also superior to placebo. In addition, 29% of the CHANTIX group were continuously abstinent from one week after TQD through the end of treatment as compared to 12% of the placebo group and 23% of the bupropion SR group.
Similarly in Study 5, patients treated with CHANTIX had a superior rate of CO-confirmed abstinence during weeks 9 through 12 (44%) compared to patients treated with bupropion SR (30%) or placebo (18%). The bupropion SR quit rate was also superior to placebo. In addition, 29% of the CHANTIX group were continuously abstinent from one week after TQD through the end of treatment as compared to 11% of the placebo group and 21% of the bupropion SR group.
Figure 1: Continuous Abstinence, Weeks 9 through 12 |
 |
| CHANTIX 0.5 mg BID | CHANTIX 1 mg BID | CHANTIX Flexible | Bupropion SR | Placebo | |
|---|---|---|---|---|---|
| BID = twice daily | |||||
Study 2 | 45% | 51% | 12% | ||
Study 3 | 40% | 12% | |||
Study 4 | 44% | 30% | 17% | ||
Study 5 | 44% | 30% | 18% | ||
14.2 Urge to Smoke
Based on responses to the Brief Questionnaire of Smoking Urges and the Minnesota Nicotine Withdrawal scale "urge to smoke" item, CHANTIX reduced urge to smoke compared to placebo.
14.3 Long-Term Abstinence
Studies 1 through 5 included 40 weeks of post-treatment follow-up. In each study, CHANTIX-treated patients were more likely to maintain abstinence throughout the follow-up period than were patients treated with placebo (Figure 2, Table 8).
Figure 2: Continuous Abstinence, Weeks 9 through 52 |
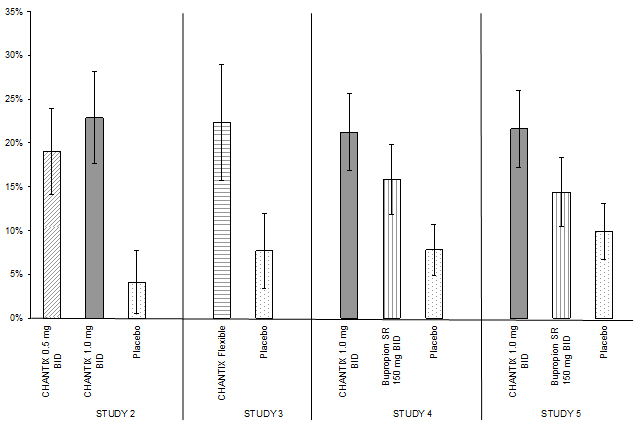 |
| CHANTIX 0.5 mg BID | CHANTIX 1 mg BID | CHANTIX Flexible | Bupropion SR | Placebo | |
|---|---|---|---|---|---|
| BID = twice daily | |||||
Study 2 | 19% | 23% | 4% | ||
Study 3 | 22% | 8% | |||
Study 4 | 21% | 16% | 8% | ||
Study 5 | 22% | 14% | 10% | ||
Study 6
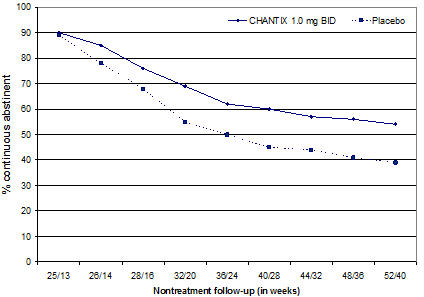
This study assessed the effect of an additional 12 weeks of CHANTIX therapy on the likelihood of long-term abstinence. Patients in this study (N=1927) were treated with open-label CHANTIX 1 mg twice daily for 12 weeks. Patients who had stopped smoking for at least a week by Week 12 (N= 1210) were then randomized to double-blind treatment with CHANTIX (1 mg twice daily) or placebo for an additional 12 weeks and then followed for 28 weeks post-treatment.
The Continuous Abstinence Rate from Week 13 through Week 24 was higher for patients continuing treatment with CHANTIX (70%) than for patients switching to placebo (50%). Superiority to placebo was also maintained during 28 weeks post-treatment follow-up (CHANTIX 54% versus placebo 39%).
In Figure 3 below, the x-axis represents the study week for each observation, allowing a comparison of groups at similar times after discontinuation of CHANTIX; post-CHANTIX follow-up begins at Week 13 for the placebo group and Week 25 for the CHANTIX group. The y-axis represents the percentage of patients who had been abstinent for the last week of CHANTIX treatment and remained abstinent at the given timepoint.
Figure 3: Continuous Abstinence Rate during Nontreatment Follow-Up |
 |
14.4 Alternative Instructions for Setting a Quit Date
CHANTIX was evaluated in a double-blind, placebo-controlled trial where patients were instructed to select a target quit date between Day 8 and Day 35 of treatment. Subjects were randomized 3:1 to CHANTIX 1 mg twice daily (N=486) or placebo (N=165) for 12 weeks of treatment and followed for another 12 weeks post-treatment. Patients treated with CHANTIX had a superior rate of CO-confirmed abstinence during weeks 9 through 12 (54%) compared to patients treated with placebo (19%) and from weeks 9 through 24 (35%) compared to subjects treated with placebo (13%).
14.5 Gradual Approach to Quitting Smoking
CHANTIX was evaluated in a 52-week double-blind placebo-controlled study of 1,510 subjects who were not able or willing to quit smoking within four weeks, but were willing to gradually reduce their smoking over a 12 week period before quitting. Subjects were randomized to either CHANTIX 1 mg twice daily (N=760) or placebo (N=750) for 24 weeks and followed up post-treatment through week 52. Subjects were instructed to reduce the number of cigarettes smoked by at least 50 percent by the end of the first four weeks of treatment, followed by a further 50 percent reduction from week four to week eight of treatment, with the goal of reaching complete abstinence by 12 weeks. After the initial 12-week reduction phase, subjects continued treatment for another 12 weeks. Subjects treated with CHANTIX had a significantly higher Continuous Abstinence Rate compared with placebo at weeks 15 through 24 (32% vs. 7%) and weeks 15 through 52 (24% vs. 6%).
14.6 Re-Treatment Study
CHANTIX was evaluated in a double-blind, placebo-controlled trial of patients who had made a previous attempt to quit smoking with CHANTIX, and either did not succeed in quitting or relapsed after treatment. Subjects were randomized 1:1 to CHANTIX 1 mg twice daily (N=249) or placebo (N=245) for 12 weeks of treatment and followed for 40 weeks post-treatment. Patients included in this study had taken CHANTIX for a smoking-cessation attempt in the past (for a total treatment duration of a minimum of two weeks), at least three months prior to study entry, and had been smoking for at least four weeks.
Patients treated with CHANTIX had a superior rate of CO-confirmed abstinence during weeks 9 through 12 (45%) compared to patients treated with placebo (12%) and from weeks 9 through 52 (20%) compared to subjects treated with placebo (3%).
| Weeks 9 through 12 | Weeks 9 through 52 | |||
|---|---|---|---|---|
| CHANTIX 1 mg BID | Placebo | CHANTIX 1 mg BID | Placebo | |
| BID = twice daily | ||||
Re-treatment Study | 45% | 12% | 20% | 3% |
14.7 Subjects with Chronic Obstructive Pulmonary Disease
CHANTIX was evaluated in a randomized, double-blind, placebo-controlled study of subjects aged ≥ 35 years with mild-to-moderate COPD with post-bronchodilator FEV1/FVC <70% and FEV1 ≥ 50% of predicted normal value. Subjects were randomized to CHANTIX 1 mg twice daily (N=223) or placebo (N=237) for a treatment of 12 weeks and then were followed for 40 weeks post-treatment. Subjects treated with CHANTIX had a superior rate of CO-confirmed abstinence during weeks 9 through 12 (41%) compared to subjects treated with placebo (9%) and from week 9 through 52 (19%) compared to subjects treated with placebo (6%).
| Weeks 9 through 12 | Weeks 9 through 52 | |||
|---|---|---|---|---|
| CHANTIX 1 mg BID | Placebo | CHANTIX 1 mg BID | Placebo | |
| BID = twice daily | ||||
COPD Study | 41% | 9% | 19% | 6% |
14.8 Subjects with Cardiovascular Disease and Other Cardiovascular Analyses
CHANTIX was evaluated in a randomized, double-blind, placebo-controlled study of subjects aged 35 to 75 years with stable, documented cardiovascular disease (diagnoses other than, or in addition to, hypertension) that had been diagnosed for more than 2 months. Subjects were randomized to CHANTIX 1 mg twice daily (N=353) or placebo (N=350) for a treatment period of 12 weeks and then were followed for 40 weeks post-treatment. Subjects treated with CHANTIX had a superior rate of CO-confirmed abstinence during weeks 9 through 12 (47%) compared to subjects treated with placebo (14%) and from week 9 through 52 (20%) compared to subjects treated with placebo (7%).
| Weeks 9 through 12 | Weeks 9 through 52 | |||
|---|---|---|---|---|
| CHANTIX 1 mg BID | Placebo | CHANTIX 1 mg BID | Placebo | |
| BID = twice daily | ||||
CVD Study | 47% | 14% | 20% | 7% |
In this study, all-cause and CV mortality was lower in patients treated with CHANTIX, but certain nonfatal CV events occurred more frequently in patients treated with CHANTIX than in patients treated with placebo [see Warnings and Precautions (5.5), Adverse Reactions (6.1)]. Table 12 below shows mortality and the incidence of selected nonfatal serious CV events occurring more frequently in the CHANTIX arm compared to the placebo arm. These events were adjudicated by an independent blinded committee. Nonfatal serious CV events not listed occurred at the same incidence or more commonly in the placebo arm. Patients with more than one CV event of the same type are counted only once per row. Some of the patients requiring coronary revascularization underwent the procedure as part of management of nonfatal MI and hospitalization for angina.
| Mortality and Cardiovascular Events | CHANTIX (N=353) n (%) | Placebo (N=350) n (%) |
|---|---|---|
Mortality (Cardiovascular and All-cause up to 52 weeks) | ||
Cardiovascular | 1 (0.3) | 2 (0.6) |
All-cause | 2 (0.6) | 5 (1.4) |
| ||
Nonfatal Cardiovascular Events (rate on CHANTIX > Placebo) | ||
Up to 30 days after treatment | ||
Nonfatal myocardial infarction | 4 (1.1) | 1 (0.3) |
Nonfatal Stroke | 2 (0.6) | 0 (0) |
Beyond 30 days after treatment and up to 52 weeks | ||
Nonfatal myocardial infarction | 3 (0.8) | 2 (0.6) |
Need for coronary revascularization | 7 (2.0) | 2 (0.6) |
Hospitalization for angina pectoris | 6 (1.7) | 4 (1.1) |
Transient ischemia attack | 1 (0.3) | 0 (0) |
New diagnosis of peripheral vascular disease (PVD) or admission for a PVD procedure | 5 (1.4) | 2 (0.6) |
Following the CVD study, a meta-analysis of 15 clinical trials of ≥12 weeks treatment duration, including 7002 patients (4190 CHANTIX, 2812 placebo), was conducted to systematically assess the CV safety of CHANTIX. The study in patients with stable CV disease described above was included in the meta-analysis. There were lower rates of all-cause mortality (CHANTIX 6 [0.14%]; placebo 7 [0.25%]) and CV mortality (CHANTIX 2 [0.05%]; placebo 2 [0.07%]) in the CHANTIX arms compared with the placebo arms in the meta-analysis.
The key CV safety analysis included occurrence and timing of a composite endpoint of Major Adverse Cardiovascular Events (MACE), defined as CV death, nonfatal MI, and nonfatal stroke. These events included in the endpoint were adjudicated by a blinded, independent committee. Overall, a small number of MACE occurred in the trials included in the meta-analysis, as described in Table 13. These events occurred primarily in patients with known CV disease.
| CHANTIX N=4190 | Placebo N=2812 | |
|---|---|---|
| ||
MACE cases, n (%) | 13 (0.31%) | 6 (0.21%) |
Patient-years of exposure | 1316 | 839 |
Hazard Ratio (95% CI) | ||
1.95 (0.79, 4.82) | ||
Rate Difference per 1,000 patient-years (95% CI) | ||
6.30 (-2.40, 15.10) | ||
The meta-analysis showed that exposure to CHANTIX resulted in a hazard ratio for MACE of 1.95 (95% confidence interval from 0.79 to 4.82) for patients up to 30 days after treatment; this is equivalent to an estimated increase of 6.3 MACE events per 1,000 patient-years of exposure. The meta-analysis showed higher rates of CV endpoints in patients on CHANTIX relative to placebo across different time frames and pre-specified sensitivity analyses, including various study groupings and CV outcomes. Although these findings were not statistically significant they were consistent. Because the number of events was small overall, the power for finding a statistically significant difference in a signal of this magnitude is low.
Additionally, a cardiovascular endpoint analysis was added to the postmarketing neuropsychiatric safety outcome study along with a non-treatment extension, [see Warnings and Precautions (5.5), Adverse Reactions (6.1), Clinical Studies (14.10)].
14.9 Subjects with Major Depressive Disorder
CHANTIX was evaluated in a randomized, double-blind, placebo-controlled study of subjects aged 18 to 75 years with major depressive disorder without psychotic features (DSM-IV TR). If on medication, subjects were to be on a stable antidepressant regimen for at least two months. If not on medication, subjects were to have experienced a major depressive episode in the past 2 years, which was successfully treated. Subjects were randomized to CHANTIX 1 mg twice daily (N=256) or placebo (N=269) for a treatment of 12 weeks and then followed for 40 weeks post-treatment. Subjects treated with CHANTIX had a superior rate of CO-confirmed abstinence during weeks 9 through 12 (36%) compared to subjects treated with placebo (16%) and from week 9 through 52 (20%) compared to subjects treated with placebo (10%).
| Weeks 9 through 12 | Weeks 9 through 52 | |||
|---|---|---|---|---|
| CHANTIX 1 mg BID | Placebo | CHANTIX 1 mg BID | Placebo | |
| BID = twice daily | ||||
MDD Study | 36% | 16% | 20% | 10% |
14.10 Postmarketing Neuropsychiatric Safety Outcome Trial
CHANTIX was evaluated in a randomized, double-blind, active and placebo-controlled trial that included subjects without a history of psychiatric disorder (non-psychiatric cohort, N=3912) and with a history of psychiatric disorder (psychiatric cohort, N=4003). Subjects aged 18–75 years, smoking 10 or more cigarettes per day were randomized 1:1:1:1 to CHANTIX 1 mg BID, bupropion SR 150 mg BID, NRT patch 21 mg/day with taper or placebo for a treatment period of 12 weeks; they were then followed for another 12 weeks post-treatment. [See Warnings and Precautions (5.1)]
A composite safety endpoint intended to capture clinically significant neuropsychiatric (NPS) adverse events included the following NPS adverse events: anxiety, depression, feeling abnormal, hostility, agitation, aggression, delusions, hallucinations, homicidal ideation, mania, panic, paranoia, psychosis, irritability, suicidal ideation, suicidal behavior or completed suicide.
As shown in Table 15, the use of CHANTIX, bupropion, and NRT in the non-psychiatric cohort was not associated with an increased risk of clinically significant NPS adverse events compared with placebo. Similarly, in the non-psychiatric cohort, the use of CHANTIX was not associated with an increased risk of clinically significant NPS adverse events in the composite safety endpoint compared with bupropion or NRT.
| CHANTIX (N=975) n (%) | Bupropion (N=968) n (%) | NRT (N=987) n (%) | Placebo (N=982) n (%) | |
|---|---|---|---|---|
Clinically Significant NPS | 30 (3.1) | 34 (3.5) | 33 (3.3) | 40 (4.1) |
Serious NPS | 1 (0.1) | 5 (0.5) | 1 (0.1) | 4 (0.4) |
Psychiatric Hospitalizations | 1 (0.1) | 2 (0.2) | 0 (0.0) | 1 (0.1) |
As shown in Table 16, there were more clinically significant NPS adverse events reported in patients in the psychiatric cohort in each treatment group compared with the non-psychiatric cohort. The incidence of events in the composite endpoint was higher for each of the active treatments compared to placebo: Risk Differences (RDs) (95%CI) vs placebo were 2.7% (-0.05, 5.4) for CHANTIX, 2.2% (-0.5, 4.9) for bupropion, and 0.4% (-2.2, 3.0) for NRT transdermal nicotine.
| CHANTIX (N=1007) n (%) | Bupropion (N=1004) n (%) | NRT (N=995) n (%) | Placebo (N=997) n (%) | |
|---|---|---|---|---|
Clinically Significant NPS | 123 (12.2) | 118 (11.8) | 98 (9.8) | 95 (9.5) |
Serious NPS | 6 (0.6) | 8 (0.8) | 4 (0.4) | 6 (0.6) |
Psychiatric hospitalizations | 5 (0.5) | 8 (0.8) | 4 (0.4) | 2 (0.2) |
There was one completed suicide, which occurred during treatment in a patient treated with placebo in the non-psychiatric cohort. There were no completed suicides reported in the psychiatric cohort.
In both cohorts, subjects treated with CHANTIX had a superior rate of CO-confirmed abstinence during weeks 9 through 12 and 9 through 24 compared to subjects treated with bupropion, nicotine patch and placebo.
| CHANTIX 1 mg BID | Bupropion SR 150 mg BID | NRT 21 mg/day with taper | Placebo | |
|---|---|---|---|---|
| BID = twice daily | ||||
Weeks 9 through 12 | ||||
Non-Psychiatric Cohort | 38% | 26% | 26% | 14% |
Psychiatric Cohort | 29% | 19% | 20% | 11% |
Weeks 9 through 24 | ||||
Non-Psychiatric Cohort | 25% | 19% | 18% | 11% |
Psychiatric Cohort | 18% | 14% | 13% | 8% |
Cardiovascular Outcome Analysis
To obtain another source of data regarding the CV risk of CHANTIX, a cardiovascular endpoint analysis was added to the postmarketing neuropsychiatric safety outcome study along with a non-treatment extension. In the parent study (N=8027), subjects aged 18–75 years, smoking 10 or more cigarettes per day were randomized 1:1:1:1 to CHANTIX 1 mg BID, bupropion SR 150 mg BID, nicotine replacement therapy (NRT) patch 21 mg/day or placebo for a treatment period of 12 weeks; they were then followed for another 12 weeks post-treatment. The extension study enrolled 4590 (57.2%) of the 8027 subjects who were randomized and treated in the parent study and followed them for additional 28 weeks. Of all treated subjects, 1743 (21.7%) had a medium CV risk and 640 (8.0%) had a high CV risk, as defined by Framingham score. Note that one site from the parent study was excluded in the assessment of CV safety and two sites were excluded in the assessment of neuropsychiatric safety.
The primary CV endpoint was the time to major adverse CV event (MACE), defined as CV death, nonfatal myocardial infarction or nonfatal stroke during treatment. Deaths and CV events were adjudicated by a blinded, independent committee. Table 18 below shows the incidence of MACE and Hazard Ratios compared to placebo for all randomized subjects exposed to at least 1 partial dose of study treatment in the parent study.
| CHANTIX N=2006 | Bupropion N=1997 | NRT N=2017 | Placebo N=2007 | |
|---|---|---|---|---|
| [IR] indicates incidence rate per 1000 person-years | ||||
During treatment* | ||||
MACE, n [IR] | 1 [2.4] | 2 [4.9] | 1 [2.4] | 4 [9.8] |
Hazard Ratio (95% CI) vs. placebo | 0.24 | 0.49 | 0.24 | |
Through end of study† | ||||
MACE, n [IR] | 3 [2.1] | 9 [6.3] | 6 [4.3] | 8 [5.7] |
Hazard Ratio (95% CI) vs. placebo | 0.36 | 1.09 | 0.74 | |
For this study, MACE+ was defined as any MACE or a new onset or worsening peripheral vascular disease (PVD) requiring intervention, a need for coronary revascularization, or hospitalization for unstable angina. Incidence rates of MACE+ and all-cause mortality for all randomized subjects exposed to at least 1 partial dose of study treatment in the parent study are shown for all treatment groups during treatment, and through end of study in the Table 19 below.
| CHANTIX N=2006 | Bupropion N=1997 | NRT N=2017 | Placebo N=2007 | |
|---|---|---|---|---|
| [IR] indicates incidence rate per 1000 person-years | ||||
During treatment* | ||||
MACE+, n [IR] | 5 [12.1] | 4 [9.9] | 2 [4.8] | 5 [12.2] |
All-cause deaths, n [IR] | 0 | 2 [4.9] | 0 | 2 [4.9] |
Through end of study† | ||||
MACE+, n [IR] | 10 [6.9] | 15 [10.5] | 10 [7.1] | 12 [8.6] |
All-cause deaths, n [IR] | 2 [1.4] | 4 [2.8] | 3 [2.1] | 4 [2.9] |
The number of subjects who experienced MACE, MACE+ and all-cause death was similar or lower among patients treated with CHANTIX than patients treated with placebo. The number of events observed overall was too low to distinguish meaningful differences between the treatment arms.
MEDICATION GUIDE
| This Medication Guide has been approved by the U.S. Food and Drug Administration. Revised: 6/2025 | |||
MEDICATION GUIDE | |||
What is the most important information I should know about CHANTIX? When you try to quit smoking, with or without CHANTIX, you may have symptoms that may be due to nicotine withdrawal, including: | |||
|
|
| |
Some people have even experienced suicidal thoughts when trying to quit smoking without medication. Sometimes quitting smoking can lead to worsening of mental health problems that you already have, such as depression. Some people have had serious side effects while taking CHANTIX to help them quit smoking, including: New or worse mental health problems, such as changes in behavior or thinking, aggression, hostility, agitation, depressed mood, or suicidal thoughts or actions. Some people had these symptoms when they began taking CHANTIX, and others developed them after several weeks of treatment, or after stopping CHANTIX. These symptoms happened more often in people who had a history of mental health problems before taking CHANTIX, than in people without a history of mental health problems. Stop taking CHANTIX and call your healthcare provider right away if you, your family, or caregiver notice any of these symptoms. Work with your healthcare provider to decide whether you should continue to take CHANTIX. In many people, these symptoms went away after stopping CHANTIX, but in some people symptoms continued after stopping CHANTIX. It is important for you to follow-up with your healthcare provider until your symptoms go away. Before taking CHANTIX, tell your healthcare provider if you have ever had depression or other mental health problems. You should also tell your healthcare provider about any symptoms you had during other times you tried to quit smoking, with or without CHANTIX. | |||
What is CHANTIX? CHANTIX is a prescription medicine to help people stop smoking. Quitting smoking can lower your chances of having lung disease, heart disease or getting certain types of cancer that are related to smoking. CHANTIX has not been shown to be effective in children 16 years of age and under. CHANTIX should not be used in children 16 years of age and under. It is not known if CHANTIX is safe and effective when used with other stop smoking medicines. | |||
Who should not take CHANTIX? Do not take CHANTIX if you have had a serious allergic or skin reaction to CHANTIX. Symptoms may include:
| |||
|
|
| |
What should I tell my healthcare provider before taking CHANTIX? See "What is the most important information I should know about CHANTIX?" Before you take CHANTIX, tell your healthcare provider if you:
Tell your healthcare provider about all the medicines you take, including prescription and over-the-counter medicines, vitamins and herbal supplements. Your healthcare provider may need to change the dose of some of your medicines when you stop smoking. You should not use CHANTIX while using other medicines to quit smoking. Tell your healthcare provider if you use other treatments to quit smoking. Know the medicines you take. Keep a list of them with you to show your healthcare provider and pharmacist when you get a new medicine. | |||
How should I take CHANTIX?
| |||
Weeks 1 through 4 | Reduce your smoking to reach one-half of your starting daily number of cigarettes. Example: If you usually smoke 20 cigarettes each day, reduce your smoking to 10 cigarettes each day during weeks 1 through 4. | ||
Weeks 5 through 8 | Reduce your smoking to reach one-quarter of your starting daily number of cigarettes. Example: If you usually smoked 20 cigarettes each day, reduce your smoking to 5 cigarettes each day during weeks 5 through 8. | ||
Weeks 9 through 12 | Keep reducing your smoking until you are no longer smoking (you reach zero cigarettes each day). | ||
Aim to quit by the end of the 12th week of treatment, or sooner if you feel ready. Continue to take CHANTIX for another 12 weeks, for a total of 24 weeks of treatment. Starting CHANTIX before your quit date gives CHANTIX time to build up in your body. You can keep smoking during this time. Take CHANTIX exactly as prescribed by your healthcare provider. | |||
| |||
Day 1 to Day 3 |
| ||
Day 4 to Day 7 |
| ||
Day 8 to end of treatment |
| ||
| |||
What should I avoid while taking CHANTIX?
| |||
|
| ||
What are the possible side effects of CHANTIX? Serious side effects of CHANTIX may include:
Stop taking CHANTIX and get medical help right away if you have any of the following symptoms:
The most common side effects of CHANTIX include:
Tell your healthcare provider about side effects that bother you or that do not go away. These are not all the side effects of CHANTIX. Ask your healthcare provider or pharmacist for more information. Call your doctor for medical advice about side effects. You may report side effects to FDA at 1-800-FDA-1088. | |||
How should I store CHANTIX?
| |||
General information about the safe and effective use of CHANTIX Medicines are sometimes prescribed for purposes other than those listed in a Medication Guide. Do not use CHANTIX for a condition for which it was not prescribed. Do not give your CHANTIX to other people, even if they have the same symptoms that you have. It may harm them. If you would like more information, talk with your healthcare provider. You can ask your healthcare provider or pharmacist for information about CHANTIX that is written for healthcare professionals. For more information about CHANTIX and tips on how to quit smoking, go to www.CHANTIX.com or call 1-877-242-6849. If you are motivated to quit smoking and did not succeed during prior CHANTIX treatment for reasons other than side effects, or if you returned to smoking after treatment, speak with your healthcare provider about whether another course of CHANTIX therapy may be right for you. | |||
What are the ingredients in CHANTIX? Active ingredient: varenicline tartrate Inactive ingredients: microcrystalline cellulose, anhydrous dibasic calcium phosphate, croscarmellose sodium, colloidal silicon dioxide, magnesium stearate, Opadry® White (for 0.5 mg), Opadry® Blue (for 1 mg), and Opadry® Clear.  LAB-0328-18.0 | |||
Additional Resources
Chat online with Pfizer Medical Information regarding your inquiry on a Pfizer medicine or vaccine.
Speak with a Pfizer Medical Information Professional regarding your Pfizer medicine or vaccine inquiry.
Available 9AM-5PM ET Monday to Friday; excluding holidays.
Submit a medical question for a Pfizer medicine or a vaccine.
The submission will be reviewed during our standard business hours.
To report an adverse event related to a Pfizer product and you are not part of a clinical trial* for this medication, click the link below to submit your information:
Pfizer Safety Reporting Site
*If you are involved in a clinical trial for either product, adverse events should be reported to your coordinating study site.
If you cannot use the above website to report an adverse event related to a Pfizer medication, please call (800) 438-1985.
You may also contact the U.S. Food and Drug Administration (FDA) directly to report adverse events or product quality concerns either online at www.fda.gov/medwatch or by calling (800) 332-1088.